One of the largest anesthesia groups in the Midwest has won an important victory in US ex rel Donegan v. Anesthesia Associates of Kansas City, 2015 WL 3616640 (W.D. Mo., June 9, 2015), a False Claims Act (FCA) lawsuit initiated by a whistleblower several years ago. On June 9, 2015, a federal district court in Missouri granted the defendant’s motion for summary judgment, effectively ending the case unless the plaintiff or “relator” files and wins an appeal.
Donegan should be helpful to anyone defending against allegations that they billed the federal government improperly for medical services, in violation of the FCA, based on someone else’s interpretation of an ambiguous rule. In the court’s own words, “A relator ‘must show that there is no reasonable interpretation of the law that would make the allegedly false statement true.’”
This the relator, John Donegan, a CRNA formerly employed by the defendant, Anesthesia Associates of Kansas City (AAKC), failed to do. He contended that AAKC had violated the Medicare regulations (42 C.F.R. § 415.110(a)(1)) governing the so-called seven steps of medical direction and specifically the requirement that the medically-directing anesthesiologist “personally participate in the most demanding aspects of the anesthesia plan including, if applicable, induction and emergence.”
Donegan argued that “emergence” occurred in the operating room and was invariably complete before the patient arrived in the recovery room. AAKC’s anesthesiologists, like so many others around the country, frequently did not return to the operating room for emergence but instead saw the patient in recovery. Therefore, according to the complaint, the anesthesiologists’ claims for medically-directed services were fraudulent in that the anesthesiologists “virtually never personally participat[ed] in the emergence of a patient coming out of a general anesthetic in the operating room.”
To commit a violation of the FCA, however, a party must have knowingly submitted false claims. “Knowing” includes acting in “deliberate ignorance” or “reckless disregard” of the truth or falsity of the information at issue, under the statute—but making a reasonable interpretation where there is any ambiguity in the regulations is not acting with the ignorance or disregard. “Emergence” as used in the medical direction regulations is ambiguous, the court ruled, noting that it has not been defined by CMS, by ASA, by the defendants’ Medicare carrier, or in any National Coverage Determination or applicable Local Coverage Determination. The court continued:
There is no guidance from any national or state anesthesiology organization defining “emergence” because emergence is a process, and each patient is different. Some patients take longer than others to recover from the effects of anesthesia, and there are different levels of emergence. The University of Kansas Hospital, where some of AAKC's anesthesiologists and CRNAs received their education and training, teaches its anesthesiology residents and nurse anesthetist students that emergence occurs over a period of time and may take an hour or more.
Given the ambiguity of “emergence,” the defendant’s definition of the process to include the patient’s recovery in the recovery unit was plausible and the view that the regulation was satisfied by seeing the patient in the recovery room was a reasonable interpretation. It was reasonable even though:
Defendant's interpretation is opportunistic because it has a financial motive to interpret the regulation this way. Under Relator's definition of “emergence,” thousands of the procedures Defendant's anesthesiologists performed should have been billed at the lower Medical Supervision rate. But there is “no authoritative contrary interpretation” of the regulation here, and the Eighth Circuit [the federal appellate court for Missouri] has ruled that “a defendant does not act with the requisite deliberate ignorance or reckless disregard by ‘taking advantage of a disputed legal question.’“ [citations omitted] While Relator has arguably put forth a more reasonable interpretation of the regulation, this is not enough.
The opinion suggests that an alternative theory of liability might have been more successful. The relator did not assert this theory in the original or amended complaints, and the court followed standard case law in refusing to consider it. Under that theory, the anesthesiologists should have been present at extubation because that is one of the most demanding procedures in a case. The court found that the argument might have been meritorious but that it was inadmissible since it was not pled until the summary judgment stage.
Readers should take note of the “extubation” theory requiring the medically-directing anesthesiologist’s presence for that procedure—future litigants who challenge anesthesiologists’ participation in “the most demanding aspects of the anesthesia plan including, if applicable, induction and emergence” almost certainly will.
The most significant principle laid down in Donegan is of course its holding that “a defendant is not liable under the FCA if the regulation is ambiguous and its statements would be true under a reasonable interpretation of the regulation.” One attorney, A. Brian Albritton of Phelps Dunbar LLP in Tampa, summed up the impact of Donegan thus on his blog:
Donegan is a real step forward in preventing relators from exploiting ambiguities in Medicare regulations to bring a qui tam action against Medicare providers and hold them hostage if they do not settle. Of course, the Court is not saying a defendant's mistaken or opportunistic interpretation can never give rise to other civil remedies by Medicare—the government has numerous avenues other than the FCA to enforce its regulatory interpretations. Yet, civil remedies are one thing, but subjecting a defendant to harsh FCA sanctions for violating an ambiguous regulation is a whole different order of magnitude. This is especially true for Medicare providers, like the defendant in this case, who easily can bill and submit thousands of small Medicare claims and for whom the $5,500 - $11,000 penalty per Medicare claim can quickly lead to exposure for catastrophic damages if they lose. Essentially, the Court's ruling has brought common sense back to the analysis of when a false claim arises when dealing with ambiguous regulations. Now, at least in the 8th Circuit, a defendant who reasonably interprets an ambiguous regulation in the absence of a contrary authoritative regulation cannot know that its interpretation is false and thus cannot be found guilty of violating the False Claims Act.
We note in closing that the opinion in Donegan, worthy though it is, is a decision on cross-motions for summary judgment, not after trial. A trial is still possible if the relator—the estate of the named CRNA who died after commencing litigation—successfully appeals the decision. We hope that it does not do so, not just because we sympathize with the defendant anesthesia group, which has had to spend a small fortune in legal fees and lost time, but because the decision is well-reasoned and well-explained.
↧
Anesthesia Group Victorious in Whistleblower Lawsuit Based on Reasonable Interpretation of “Emergence”
↧
The SGR “Fix” in the Context of Anesthesia Practice
By:
Serene K. Zeni, Esq.
Clark Hill, PLC, Birmingham, MI
Greg Moore, Esq.
Clark Hill, PLC, Birmingham, MI
Alexandra A. Hall, Esq.
Clark Hill, PLC, Birmingham, MI
It is not by chance that the discussions leading to the SGR “fix,” the Medicare Access and CHIP Reauthorization Act of 2015 (H.R.2), signed into law on April 16, 2015, began with an anesthesiologist, Republican Congressman Andy Harris, MD. The manner in which the Sustainable Growth Rate (SGR) would be fixed was particularly relevant to anesthesiologists who get roughly 31 percent of commercial payment when they bill Medicare, according to Jane Fitch, MD, chair of anesthesiology at the University of Oklahoma Health Sciences Center in Oklahoma City, in an interview with Anesthesiology News. Understanding H.R.2, therefore, is necessary to understand how anesthesia practices will be reimbursed in the future.
To understand the rationale underlying H.R.2, it is necessary to start with the basic assumption that providers need to shift away from the fee-for-service model and that there is not already a focus on quality by the practitioner without forcing the issue through reimbursement. It will then appear that H.R.2 guides the payment system in the right direction. While the underlying concepts of quality seem simple to integrate into reimbursement, H.R.2 ignores the cost and complexity involved in instituting its measures on a provider level. Even after a provider invests in the cost of compliance, H.R.2 is broad enough that a provider can miss the mark on what it takes to qualify for an incentive or higher reimbursement.
I. The Immediate Fix
 Before Senate approval of H.R.2 on April 14, 2015, Medicare payments for physician services were annually adjusted upward or downward by a conversion factor determined by the SGR. The SGR intended to ensure the expense per Medicare beneficiary did not surpass the gross domestic product (GDP). However, due to the slow growth of the economy, SGR would have cut reimbursement for physician services by 21.2 percent by April 1, 2015.
Before Senate approval of H.R.2 on April 14, 2015, Medicare payments for physician services were annually adjusted upward or downward by a conversion factor determined by the SGR. The SGR intended to ensure the expense per Medicare beneficiary did not surpass the gross domestic product (GDP). However, due to the slow growth of the economy, SGR would have cut reimbursement for physician services by 21.2 percent by April 1, 2015.
H.R.2 avoids this massive decline by freezing the current conversion factor to zero percent through June 2015, which means physicians will maintain their current compensation for services provided. The conversion factor will increase to .5 percent as of July 1, 2015, and continue at .5 percent every year through 2019, which will gradually increase physician reimbursement every year rates are recalculated. From 2020 to 2025, the conversion rate will return to zero percent, leveling reimbursement during that period.
II . Not Catchy Enough For The Headlines
Where providers may get lost is in the actual details of reimbursement after the SGR fix is implemented. The complex reimbursement model achieved by H.R.2 did not make the headlines when the public was pressuring the Senate to sign the bill into law.
As of 2026, H.R.2 incentivizes providers towards “quality” as opposed to volume consistent with the overall trend in health care. For this purpose, H.R.2 requires use of two conversion factors, which will apply to practitioners (including physicians, physician assistants, nurse practitioners and clinical nurse specialists and certain other qualifying professionals) depending on whether they are reimbursed under a “qualifying” alternative payment model (APM). A provider qualifies by furnishing a particular threshold (depending on the year, starting in 2019) of his or her services under an APM or an entity participating in an APM that falls under one of these payment systems as defined under the Social Security Act: (1) innovative payment models; (2) the shared savings program; (3) a demonstration; or (4) any demonstration project required by federal law.
The reward for “qualifying” is reimbursement with a year upward conversion factor of .75 percent. The caveat is that he or she must also use certified electronic health record (EHR) technology and specific quality measures and either bear financial risk for participation or be a patient-centered medical home. A conversion factor of .25 percent will apply to professionals participating in non-qualifying APMs, leaving the fee-for-service model available, but, theoretically, less attractive.
H.R.2 sunsets payment incentives under the physician quality reporting, value-based payment modifier, and meaningful use programs by 2018. H.R.2 establishes in its place the Merit-based Incentive Payment System (MIPS) in 2019, merging all three programs into one. MIPS is structured to evaluate overall provider performance by scoring performance in various categories and giving each category a proportion: “quality” (30 percent), “resource use” (30 percent), “clinical practice improvement activities” (15 percent), and “meaningful use of electronic health records” (25 percent). Each measure is largely dependent on provider reporting and studies with an additional incentive for “exceptional performance.” The provider’s MIPS score will factor into her reimbursement rate.
III . Just When You Thought You Understood “Meaningful Use”
H.R.2 reestablishes the current standards for data sharing. H.R.2 mandates and permits data sharing (even selling) in multiple contexts. Of course, H.R.2 continues to promote data privacy and security while expanding access to unidentifiable patient information.
The extent of data sharing encouraged by H.R.2 increases the data security risks already prevalent in the healthcare industry. For example, H.R.2 sets a goal of achieving interoperability of EHR systems by December 31, 2018, and prohibits deliberate blocking of information sharing between EHRs from different vendors by redefining meaningful use. This requirement may pose a challenge to providers given the Secretary’s power to adjust meaningful use penalties and decertify EHRs if not achieved.
The data sharing provisions of H.R.2 will generate further complications for professionals already struggling to comply with HIPAA and HITECH.
IV . The Provider Fix
Regardless of one’s perspective on H.R.2, the practitioner must nonetheless prepare for its impact. Even if a provider chooses not to participate in Medicare, third-party payers are more than likely to follow suit and the precedent established by H.R.2 will be inescapable.
The unpredictability of the value add or decline of H.R.2 is creeping into different contexts of provider arrangements. For example, recently drafted employment contracts accommodate the contingency of a decline in reimbursement by shifting the burden of such decline from the employer to the employee.
Anesthesiologists will need to reevaluate their current efforts to comply with quality measurements, data protection and value performance. They will need to look at current and potential relationships with other providers and ensure such relationships account for the potential decline in reimbursement in the long term. H.R.2 did not simply solve the SGR problem. Rather, it created numerous long-term challenges that providers will need to truly understand to protect their bottom line and determine their professional success. It also perpetuated the many challenges already experienced by anesthesiologists in other payment reform contexts, such as failing to answer how quality is measured in the context of anesthesia practices. Despite the law starting with a conversation in the presence of anesthesiologists, the law only temporarily favors anesthesiologists and only creates more ambiguity in the long term.
↧
↧
A Role for Anesthesiologists in CMS’s New Comprehensive Care for Joint Replacement Payment Program
Most of the hospitals located in any of 75 Metropolitan Statistical Areas (MSAs) would be required to participate in a new program that bundles the payment for joint replacement surgeries under a proposal issued by CMS on July 9, 2015. As necessary members of the team that performs joint replacement surgeries, anesthesiologists in those MSAs should consider approaching their hospitals early in order to be sure of a seat at the table. And they should be prepared to share both the opportunity and the risks.
The proposed rule for the Comprehensive Care for Joint Replacement (CCJR) is a significant departure from the voluntary Bundled Payment for Care Improvement (BPCI) program in that it requires virtually all affected hospitals to be financially responsible for all of the care of these patients for 90 days after discharge. (Hospitals already participating in the BPCI program will be excluded.)
Physicians are not subject to the mandate but obviously the success of the CCJR program will depend on their participation. Participating hospitals may share CCJR savings or penalties—the latter to a maximum of 25 percent of the amount at risk—with physicians by agreement. Because the hospitals would be accountable for all Part A and Part B costs related to the episode of care, including professional charges and post-operative visits, they would have a strong incentive to seek to engage their orthopedic surgeons, anesthesiologists and other physicians involved in ensuring the quality and cost-effectiveness of the care furnished to the joint replacement patients.
Why hip and knee joint replacement procedures? In 2013, the respective Diagnosis Related Groups (DRGs) 469 and 470 were reported for some 400,000 inpatient procedures for a total Part A (hospital) cost of more than $7 billion. According to the CMS Innovation Center’s summary of the CCJR,
While some incentives exist for hospitals to avoid post-surgery complications that can result in pain, readmissions to the hospital, or protracted rehabilitative care, the quality and cost of care for these hip and knee replacement surgeries still vary greatly among providers.
For instance, the rate of complications like infections or implant failures after surgery can be more than three times higher at some facilities than others, increasing the chances that the patient may be readmitted to the hospital. And, the average Medicare expenditure for surgery, hospitalization, and recovery ranges from $16,500 to $33,000 across geographic areas.
Participating hospitals would be eligible for bonus payments in 2017 based on 2016 performance and for decreased payments only beginning in the following cycle. Each hospital would have a price target based on three years of historical cost and utilization data. The target price generally would include a two percent discount over expected episode spending.
For the first two years, the target would be a blend of hospital-specific and regional costs, transitioning to fully regional targets over the full five-year demonstration period. If the patient’s combined total Part A and Part B costs during the 90-day period following discharge were below the target price for the procedure, and the hospital achieved quality performance requirements on three specific measures, the hospital would receive a reconciliation payment from Medicare for the difference between the target price and actual episode spending, up to a cap of 20 percent. If actual costs exceeded the target, however, the hospital would be subject to a negative adjustment of up to 20 percent.
The three quality measures are:
Hospital-Level Risk-Standardized Complication Rate Following Elective Primary Total Hip Arthroplasty and/or Total Knee Arthroplasty;
Hospital-Level 30-day, All-Cause Risk-Standardized Readmission Rate Following Elective Primary Total Hip Arthroplasty and/or Total Knee Arthroplasty, and
Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) Survey.
Quality performance requirements for reconciliation payment eligibility would increase over the lifetime of the model in order to incentivize continuous improvement on these measures.
CMS will consider public comments received on the proposed rule through September 8, 2015. The final rule is expected to appear in the Federal Register around November 1st. Suzanne Delbanco and François de Brantes suggested some of the changes to the CCJR program that CMS may well consider in their criticism of the initiative published on the Health Affairs blog on August 6th (The Payment Reform Landscape: Why Medicare’s Hip And Knee Replacement Payment Model May Not Be The Answer For Other Payers And Purchasers). They noted that:
Limiting the possibilities to acute care facilities would prevent lower-cost facilities from competing in the marketplace, while “in fact, many private and public sector purchasers experimenting with episode-based or bundled payment have designated the physician as the ‘quarterback’ of the episode, not the facility." (More and more hip and knee replacement procedures are being performed in ambulatory surgery centers – Ed.)
The model should “adjust for patient severity to avoid a market-average price. Not every patient is the same; if employers and other purchasers are working hard to help enrollees stay healthy and get back to work faster, the price for their bundles should reflect that and they should not have to pay an inflated price due to the sickness or complications of other populations.”
The DRGs “targeted by the program are too broad and include procedures unrelated to replacing a hip or knee. This could contribute to higher total costs of care and result in hospitals being penalized unjustly for those unrelated procedures …. Keep the providers’ focus on what they can control by limiting the services in the bundle to those that are directly relevant to the targeted procedure.”
This recent move by CMS to require bundling of payment for hip and knee replacements is just the beginning of its efforts to link provider profits with costs and quality metrics. Observers also expect commercial insurers and providers to follow CMS's lead. Anesthesiologists should be on this train. In fact, many of those already participating in Perioperative Surgical Home activities are working toward improving costs and quality during the post-operative phase as well as during the acute period of care. We will all be studying their experience carefully.
↧
Anesthesia Group Mergers, Acquisitions and (Importantly) Alternatives
It’s come to the point that a good part of my work with anesthesia groups involves surgery: removing an earworm—a catchy tune that continually runs through the group’s mind.
In fact, it’s always the same tune, part of The Clash’s Should I Stay or Should I Go Now:
Should I stay or should I go now?
Should I stay or should I go now?
If I go, there will be trouble,
and if I stay it will be double.
So come on and let me know.
This indecision’s bugging me.
Stay, as in should our group remain independent?
Go, as in should we sell out to someone, maybe anyone, who’ll buy us?
But as is generally the case in life, the decision is not purely either/or, black or white, yes or no. There are many alternatives. And that’s what we “operate on” as part of what I call the Future FinderTM process.
Some Background
 As you’re certainly more than familiar, there’s a storm of uncertainty resulting from the rapidity of market change in healthcare in general and in anesthesiology in particular.
As you’re certainly more than familiar, there’s a storm of uncertainty resulting from the rapidity of market change in healthcare in general and in anesthesiology in particular.
Hospitals seek to employ or otherwise "align" physicians. They seek to control specialty referrals through employment models, accountable care organizations and other hospital-centric networks.
For independent anesthesia groups there’s mounting competitive pressure from large regional and national groups. And for all anesthesia providers, from the individual to the immense group, there’s the looming impact of technology.
Many believe that they will find shelter from this uncertainty through a sale to a large regional or national group, or to a private equity backed venture. Yet others are forging new routes, alone or in alliance with other practitioners, and creating their own futures.
What route is best for you?
Acquisitions
It’s important to understand the basic economic structure of an anesthesia group acquisition.
As opposed to the sale of, for example, a manufacturing business that includes inventory, machinery, raw materials and real estate, all of which can be valued and sold, the only thing that most anesthesia groups have to sell is their future cash flow.
Accordingly, the usual anesthesia practice acquisition is essentially a valuation, at a multiple, of the group’s reconstructed earnings; reconstructed because most groups don’t have significant, or any, earnings in the technical sense due to the fact that they annually distribute all of their available cash to their physician owners.
To illustrate, if the group is normally distributing $100x to the physicians when the amount of compensation required to recruit and retain is a lesser $70x, then a purchaser would, conceivably, value the group based on a multiple of the difference, that is, on a multiple of $30x.
As a part of the sale, the group’s physician owners would receive an employment contract for, in our simplified example, $70x per year, often for a guaranteed number of years.
The astute reader might realize that, all things being equal, the group has financed the purchase price by forgoing the collection of the additional $30x. That’s correct.
However, those physicians nearing the end of their active careers may be more than happy to obtain five, or six, or more times that $30x up front because they have no intention of working for more than one or two additional years.
Even those physicians who foresee many years of continued practice often favor an acquisition because it results in a shifting of risks, for example, the risks that the hospital contract might be terminated, or that collections will plummet one year into the term of a multiple year employment guarantee.
While certain risks can be shifted, sellers do assume other risks, such as the fact that continued practice, without a sale, might be more remunerative or that the lump sum purchase price received might not actually deliver a higher return than would a continued investment in their own careers.
How long the hot acquisition market will last is anyone’s guess. Certainly large groups in key markets, key being different for each potential acquirer, tend to drive higher valuations. But that’s not to say that a smaller group in a particular buyer’s viewpoint wouldn’t make a prime candidate to fill in perceived gaps in their footprint.
Alternatives
 Just because the acquisition market is hot doesn’t mean that you should be interested in a sale or, even if you are, that it’s the right option for you or that any buyer would actually purchase your group.
Just because the acquisition market is hot doesn’t mean that you should be interested in a sale or, even if you are, that it’s the right option for you or that any buyer would actually purchase your group.
And, for the many who seek to control their own future, no sale can deliver that ability. By definition, you will have sold off your ability to control your professional future, at least within the confines of the acquired group and maybe, depending on the scope and enforceability of covenants not to compete, within a significant geographic area. Maybe that trade-off is worth it to you. Maybe it’s not.
And, for those who believe that larger is smarter or that larger is safer, consider the example of General Motors’ bankruptcy.
There are multiple alternatives to a sale, some mutually exclusive and others additive. Let’s explore some of them.
1. Become a Much Better Competitor
Reminiscent of Garrison Keillor’s imaginary Lake Wobegon, “where all the women are strong, all the men are goodlooking, and all the children are above average,” I’ve yet to meet an anesthesia group that doesn’t claim that it provides wonderful care and fantastic service and that it has a great relationship with the hospital’s administration.
But, as Richard Feynman quipped, “The first principle is that you must not fool yourself—and you are the easiest person to fool.” So, begin with telling the truth.
Immediately start to take steps to cement your relationship with the facilities at which your group currently provides services. Correct service deficiencies. Correct personnel deficiencies. Create an Experience MonopolyTM in regard to the level of service that your group provides to its “customers”: hospitals, referring physicians and patients. If you receive a coverage stipend, seek ways to reduce it, knowing that that is how competitors often gain a foothold.
Explore opportunities to expand your practice to encompass additional facilities. This must include additional hospitals and, very importantly, outpatient facilities. Expansion outside of acute care hospitals is essential in order to hedge against a future that will likely not be hospital-oriented.
At the same time, tighten up your group’s internal operations. Get your governance structure in order to enable your group to make quick decisions. Review your compensation plan to make certain that it creates the proper incentives and motivators. And begin to bank capital to enable the group to expand on multiple fronts.
2. Do Your Own M&A
Instead of simply thinking of mergers and acquisitions (M&A) from the perspective of a target, consider that your group can become an acquirer.
Although you might actually consider buying another local group that is engaging in a true acquisition, there’s no reason why you need to restrain your thinking to paying cash.
Your group can combine with other groups through merger to form your own larger entity. Although size itself doesn’t secure success, it can enable your group to establish a wider geographic presence, achieve some economies of scale and potentially create stronger payer contracting power. It also serves to create leverage in connection with facility contract negotiations.
There is a plethora of ways to structure mergers, from those in which your group essentially makes itself larger by subsuming other groups into its fold, to structures in which your group and another create a new entity.
3. Alignment Models
 Within bounds permitted between competitors (although the truly entrepreneurial reader will realize that there’s no need to deal only with competitors), there’s little limit on the types of non-traditional or hybrid ventures that can be constructed.
Within bounds permitted between competitors (although the truly entrepreneurial reader will realize that there’s no need to deal only with competitors), there’s little limit on the types of non-traditional or hybrid ventures that can be constructed.
For example, it’s possible to construct co-op type ventures in which groups across geographic bounds align for purposes of reducing costs (e.g., malpractice insurance) and of amassing data that can be analyzed and used to improve their practices (e.g., through the design of protocols) as well as to demonstrate value to hospitals and health systems.
Or, as another example, it’s possible to construct management services organization (MSO) structures in which multiple groups link to centralize various management functions. There’s a mention of MSOs below, from a slightly different angle.
Note that these ventures do not have to be limited to arrangements with other anesthesia groups. Depending on the specifics, they can be cross-specialty (e.g., anesthesiology and radiology) and cross-profession (e.g., MD and CRNA).
4. Profit From Existing Capabilities and Intellectual Capital
If your group has an internal business operation with a dedicated practice manager, consider expanding that function into a separate spun off business entity that provides MSO type services to other groups as well as to your own.
For example, you can sell your manager’s and your group’s leaders’ business expertise, and you can operate a locums service with your own group’s physicians or with third parties.
Importantly, your MSO structure can be a vehicle to create initial relationships that might later be expanded to make the client a merger or acquisition target.
Conclusion
There are always more options than you’ve considered to date. There are always alternative structures to a sale and alternative strategies for the success of your practice.
Even if you’re committed to seeking a buyer, you can’t stop or even slow your efforts to develop your business while you’re searching. There might not be a buyer. If there is, you may not like the price. You might realize that you don’t want to sell. You might actually want to buy.
In closing, remember that the best strategy formulation is not a straight-line process. It’s not an on-off/sell-or-don’tsell/ merge-or-don’t-merge situation. Rather, it’s a fluid, circular process, keeping options open even as you explore a primary one, continuing to build as you continue to search for the right structure, the right deal, for you.
↧
More Alphabet Soup for Anesthesiologists, CRNAs and AAs—the Medicare QRURs
Next year, all physicians in groups of ten or more eligible professionals (EPs) will be subject to the Medicare Value-Based Payment Modifier (VM). Larger groups with 100 or more EPs are already seeing VM adjustments based on their 2013 performance.
In 2017, the VM will apply to all physicians, whether they are in solo practice or are in a group with two or more EPs. And in 2018, payments to nurse anesthetists and anesthesiologist assistants will also reflect the impact of the VM.
It is time for us to familiarize ourselves with the Physician Feedback Program and the Quality and Resource Use Reports (QRURs) that will let physicians find out how they are doing, in terms of the quality and cost metrics that will determine the VM payment adjustment, and compare themselves to their peers.
VM Recap
As we stated in our November 3, 2014 Alert (What Anesthesiologists Need to Know about the Value-Based Payment Modifier):
The VM, which was mandated by the Affordable Care Act, adjusts payments to physicians, groups of physicians, and other EPs based on the quality and cost of care they furnish to patients enrolled in the traditional Medicare Fee-for-Service program.
EPs practicing high-quality, low-cost care will earn a positive VM, while those whose scores indicate relatively lower quality and higher cost may have a negative VM. Given that the VM program is budget neutral, the amount of the positive modifier is unknown until all groups are scored. After such scoring, the aggregate adjustments applied to the low quality/high cost groups are used to fund the positive adjustment payment to the high quality/low cost groups.
CMS will calculate the VM for each practice. It is derived from a quality composite score and a cost composite score. The quality composite score summarizes the group’s (determined by Tax Identification Number or TIN) performance on quality care for Medicare beneficiaries for as many as six equally weighted quality domains: (1) Clinical Process/Effectiveness, (2) Patient and Family Engagement, (3) Population/Public Health, (4) Patient Safety, (5) Care Coordination, and (6) Efficient Use of Healthcare Resources. Each domain score is based on performance scores for PQRS measures reported, using its associated domain. The cost composite score summarizes a TIN’s performance regarding resource use for its attributed Medicare beneficiaries, across two equally weighted cost domains: Per Capita Costs for All Attributed Beneficiaries and Per Capita Costs for Beneficiaries with Specific Conditions (diabetes, CAD, COPD, and heart failure).
As of yet, there are no cost measures that can be attributed to single-specialty anesthesia groups. A beneficiary (and the beneficiary’s assigned costs) will only be attributed to an anesthesia group if that group provided the majority of the beneficiary’s primary care visits. For groups without cost measure scores, CMS will consider the group’s cost "average" for purposes of the VM adjustments.
CMS is currently applying the VM to groups with 100 or more EPs and will apply the VM to groups of ten or more EPs in 2016, based in part on 2014 PQRS participation in the Physician Quality Reporting System (PQRS). Groups of ten or more EPs that do not avoid the -2.0 percent PQRS penalty in 2014 will automatically also be subject, cumulatively, to the -2.0 percent VM penalty in 2016, applied at the claim level.
Groups that successfully report PQRS measures and thus avoid the 2014 PQRS penalty may receive an upward, neutral, or downward VM payment adjustment based on their quality and cost performance scores, as follows:
Groups of 10-99 EPs will only be subject to an upward or neutral payment adjustment in 2016 based on 2014 performance scores.
Groups of 100 or more EPs will receive an upward, neutral or downward adjustment based on performance scores. Those groups whose performance scores place them in lower quality/higher cost categories will have payment at risk under the VM of up to 2.0 percent.
Further details on the timeline for the phase-in of the VM, which began in 2013 and will be complete in 2018, are available at Timeline to Phase In the Value-Based Payment Modifier.
What Are QRURs?
The QRURs are the other primary component of the Physician Feedback Program, the VM being the first. They contain performance information on the quality and cost measures used to calculate the quality and cost composites of the VM—both individual and comparative. According to CMS, “they help physicians understand their current performance levels and how to use the information provided in the QRURs to improve their performance on quality and cost measures.”
In April 2015, CMS released the 2014 Mid-Year QRURs covering the period July 1, 2013 – June 30, 2014. The Mid-Year QRURs were made available, for informational purposes only, to every group and solo practitioner nationwide who reported at least one quality or cost measure with at least one eligible case during the performance period from January 1, 2014 to December 30, 2014. They contain information on a subset of the measures that will be used to calculate the 2016 Value Modifier.
The 2014 Annual QRURs, for the entire 2014 calendar year, are expected to be released any day. For the first time, CMS will make the Annual QRURs available for everyone, including EPs who will not be subject to the MV in 2016—groups and solo practitioners with non-physician eligible professionals only, as well as groups and solo practitioners that participated in the Shared Savings Program, the Pioneer ACO Model, or the Comprehensive Primary Care initiative in 2014.
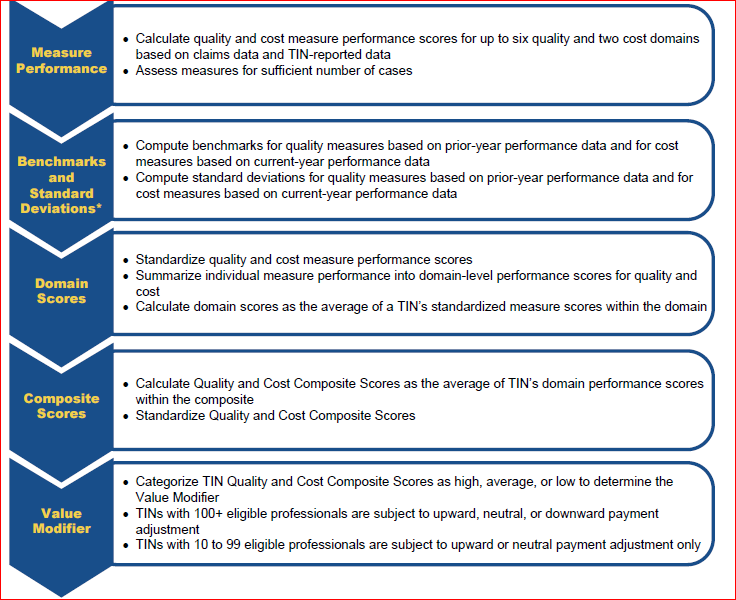
For information on the methodology behind the Annual QRURs, consult the chart below and the 81-page CMS publication in which it appears (https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeedbackProgram/Downloads/2014QRUR-2016VM-DetailedMethodology.pdf)
Methodology for Computing the VM Based on the QRURs
How to Access Your QRUR
You must obtain an Enterprise Identity Management System (EIDM) account in order to access a QRUR. Some readers may remember that they have seen references to “Individuals Authorized Access to CMS Computer Services (IACS)” accounts in connection with checking VM or PQRS reports. CMS discontinued the use of IACS accounts in mid-July and replaced them with EIDM accounts. (If you have an IACS account that you previously used to access QRURs, then follow the instructions for migrating to sign up for an EIDM account.)
You can access QRURs and PQRS Feedback Reports on behalf of a group or solo practitioner at https://portal.cms.gov. QRURs are provided for each Medicare-enrolled Taxpayer Identification Number (TIN). At least one person from your group will need to obtain an EIDM account. Preliminarily, that person must select the correct role:
- On behalf of a group practice (two or more EPs)
- Security Official role, or
- Group Representative role (the difference between the two roles is simply that the Security Official can approve requests for the Group Representative role)
- On behalf of a solo practitioner
- Individual Practitioner role, or
- Individual Practitioner Representative role (again, the Individual Practitioner has the ability to approve requests for the representative role but not vice versa).
Then, once you have an EIDM account with the correct role (for which process more detailed information can be found in CMS’s Guide for Obtaining a New EIDM Account with a ‘Physician Quality and Value Programs’ Role), follow the step-by-step instructions provided in the latest CMS Reference Guide for Accessing the QRURs. At press time, only the Quick Reference Guide for Accessing the 2014 Mid-Year QRURs and Supplementary Exhibits was available. Although the information in the guide for the Annual QRURs will probably be quite similar, certain key information such as the “Calculations related to the VM, including, cost and quality composite scores, quality and cost performance categories (High, Average, Low), and the quality tiering categories” will only appear in the Guide for the Annual QRURs—which CMS is expected to publish shortly. We will notify you once that Guide is available.
Until now, the VM and the QRURs have only affected Medicare payments to large groups of 100 or more EPs. Beginning on January 1, 2016, however, the VM will apply to Fee-For-Service payments for physicians in groups of 10 or more EPs based on performance in 2014.
In the Fall of 2016, for all groups and solo practitioners nationwide, CMS will release QRURs based on quality and cost data from CY 2015. The reports will show the 2017 Value Modifier payment adjustment under the PFS for all physician solo practitioners and physicians in groups with 2 or more EPs. In 2017, all physicians will be subject to the VM, and in 2018, all EPs—including by definition CRNAs and AAs—may also see their Medicare payments adjusted through the VM.
Because of this timeline, we encourage all anesthesia personnel to obtain and understand their QRURs as soon as the 2014 Annual reports are available.
↧
↧
Anesthesia Practices Are Not Islands
“No man is an island, entire of itself; every man is a piece of the continent, a part of the main” begins John Donne’s famous poem. Anesthesiologists have come to realize that not only are they “a piece of the continent” that is their group, but that they are interdependent on their hospital or health system. The anesthesiologist’s and the group’s well-being is bound up with that of their institution, and perhaps with the health and welfare of other entities as well.
The hospital “continent” is under enormous pressure to improve quality and to hold down costs, and so, therefore, is the “country” that is the anesthesia department. If the incumbent anesthesia groups are not properly managing their costs and quality, the chances are that their hospitals are looking for alternatives. ABC Vice President Jody Locke’s latest article for the Communiqué, Why Utilization and Productivity Metrics Matter, walks readers through the variety of metrics available to practices that want to measure and demonstrate their value to their hospital partners. The immediate goals are to develop data that lead to more efficient coverage models in terms of both staff and operating room utilization and to identification of best practices—including productivity— among the providers. As Mr. Locke writes, “Those who have come to understand the importance of being lean and effective are gaining market share while those that refuse to accept the inevitable are losing ground and losing their franchises. Effectiveness and efficiency are the new keys to success.” The overarching goal is to produce the lean, cost-effective and high-quality anesthesia service demanded of the hospital’s anesthesia partners.
Groups can form bigger islands, or even continents of their own, by growing. Mergers and acquisitions are the more popular and certainly the more immediate strategy, but organic growth is often feasible as well, as Mark Weiss, Esq. writes in Anesthesia Group Mergers, Acquisitions and (Importantly) Alternatives—and it entails becoming a more valuable component of the hospital continent or family. Cement your current facility relationships, explore opportunities to expand the practice to additional facilities and tighten up the group’s internal operations. Other alternatives to being acquired by a larger entity include acquiring another group, creating a cooperative arrangement with other practices or launching a Management Services Organization (MSO), or even offering a practice management or locums service.
“Even if you’re committed to seeking a buyer,” states Mr. Weiss, “you can’t stop or even slow your efforts to develop your business while you’re searching.” Bill Britton of Cross Keys Capital elaborates on this point in How an Investment Banker Can Make an Anesthesia Practice That Wants to Sell Become a More Attractive Acquisition Partner. As we know, some groups are solving the dilemma of small size and limited resources by seeking out venture capital. In his article, Mr. Britton identifies seven areas that buyers of anesthesia practices focus on, starting, not surprisingly, with corporate governance and leadership. The characteristics that make a group an attractive target are also the characteristics that make it successful. The investment banker’s perspective is one that everyone should consider.
Did you miss the death story of the Medicare Sustainable Growth Rate (SGR) formula? Attorneys Serene Zeni, Gregory Moore and Alexandra Hall explain its history and the legislation that killed the SGR, as well as what comes next, in The SGR “Fix” in the Context of Anesthesia Practice.
As health plan co-insurance and deductible amounts continue to grow, so do the challenges of collecting. “Self-pay” used to refer primarily to uninsured patients. As Neda Ryan, Esq. and Christopher Ryan, Esq. explain in Getting Paid by the Self-Pay Patient, the term now applies, too, to patients with high deductibles. Obtaining compensation from these individuals often depends on having in place the necessary policies and protocols, which are summarized in the article.
Has Someone Gotten in Trouble for Doing That? asks Vicky Mykowiac, Esq. Yes, someone has, and Ms. Mykowiac explains various problematic activities that gave rise to civil and criminal fraud actions with Lessons for Anesthesia Groups from Real Cases and lessons learned. One specific area of interest on the part of the federal government is physician compensation that may implicate the anti-kickback statute. ABC Vice President Joette Derricks reviews recent fraud alerts in Is the Office of the Inspector General Turning its Attention to Physician Issues?
We are well into the second half of 2015 and it seems that the anesthesia practice management news cycle is running faster than ever. Groups continue to morph and consolidate, as do health systems and, more recently, even large health plans. We hope that our publications continue to provide a useful service in helping our readers navigate these many changes.
↧
What is a Valid Anesthesiologist’s Signature on a Medical Record, and What Does it Mean?
What does it mean when an anesthesiologist signs a patient’s medical record? What happens if the anesthesiologist’s signature is missing?
In general, a signature has three basic purposes:
Intent. The signature indicates confirmation that the signing party reviewed and approved the content or that s/he authored the document and approved the content.
Integrity. The signature protects the integrity of the document against a claim that the entry was invalid or that it had been altered.
Identity. The signature identifies the signing party.
In the healthcare context, for medical review purposes, Medicare requires that the treating or ordering practitioner authenticate the services in question, with very few exceptions. The method used must be a handwritten or electronic signature. (Program Integrity Manual Chapter 3 Section 3.3.2.4)
The point of the practitioner’s signature in patients’ medical records, operative reports, anesthesia records, orders and, test findings is to demonstrate that services reported to Medicare have been accurately and fully documented, reviewed and authenticated. Furthermore, it confirms the provider has certified the medical necessity and reasonableness for the service(s) submitted to the Medicare program for payment consideration.
The exceptions to the authentication requirement are:
Facsimiles of original written or electronic signatures are acceptable for the certifications of terminal illness for hospice.
There are some circumstances for which an order does not need to be signed. For example, orders for some clinical diagnostic tests are not required to be signed and for which a progress note can adequately show the physician’s intent.
Signature requirements in specific, relevant regulations or Medicare policies or manuals take precedence over general principles.
Practitioners with physical disabilities preventing them from signing may use rubber stamps.
The Program Integrity Manual and the Medicare Learning Network fact sheet “Complying with Medicare Signature Requirements” provides ample detail on the types of signatures that are, and are not, acceptable.
Handwritten Signatures – Acceptable
Legible full signature
Legible first initial and last name
Illegible signature over a typed or printed name
Illegible signature where the letterhead, addressograph or other information on the page indicates the identity of the signing provider. Example: An illegible signature appears on a prescription. The letterhead of the prescription lists three physicians’ names. One of the names is circled.
Illegible signature not over a typed/printed name and not on letterhead, but the submitted documentation is accompanied by: 1) a signature log, or 2) an attestation statement
Initials over a typed or printed name
Initials not over a typed/printed name but accompanied by: 1) a signature log, or 2) an attestation statement
Unsigned handwritten note where other entries on the same page in the same handwriting are signed
Electronic Signatures – Acceptable
The Program Integrity Manual validates the use of electronic signatures, but warns physicians and others that:
Providers using electronic systems need to recognize that there is a potential for misuse or abuse with alternate signature methods. For example, providers need a system and software products that are protected against modification, etc., and should apply adequate administrative procedures that correspond to recognized standards and laws. The individual whose name is on the alternate signature method and the provider bear the responsibility for the authenticity of the information for which an attestation has been provided. Physicians are encouraged to check with their attorneys and malpractice insurers concerning the use of alternative signature methods.
Examples of acceptable electronic signatures include the following, taken from Palmetto GBA’s “Medicare Medical Records: Signature Requirements, Acceptable and Unacceptable Practices:”
Chart 'Accepted by' with provider’s name
'Electronically signed by' with provider’s name
'Verified by' with provider’s name
'Reviewed by' with provider’s name
'Released by' with provider’s name
'Signed by' with provider’s name
'Signed before import by' with provider’s name
'Signed: John Smith, M.D.' with provider’s name
Digitized signature: Handwritten and scanned into the computer
'This is an electronically verified report by John Smith, M.D.'
'Authenticated by John Smith, M.D'
'Authorized by: John Smith, M.D'
'Digital Signature: John Smith, M.D'
'Confirmed by' with provider’s name
'Closed by' with provider’s name
'Finalized by' with provider’s name
'Electronically approved by' with provider’s name
'Signature Derived from Controlled Access Password'
If the signature on the medical record or order is unacceptable, because, for example, it is on an unsigned typed note without the physician’s typed or printed name, or because the record merely indicates “signature on file,” the Medicare contractor will contact the provider or billing entity and give them 20 days to submit an attestation statement or signature log (unless the claim is to be denied independently, for reasons unrelated to signature requirements.)
A signature log can be created at any time. It may be an individual log or a group log and is a typed listing of the provider(s) identifying their name with a corresponding handwritten signature.
An attestation is a declaration submitted to authenticate an illegible or missing signature on medical documentation. To be valid for Medicare, it must include: (a) the printed full name of the physician or other practitioner, (b) sufficient information to identify the beneficiary, (c) the date of service (d) the signature of the physician or practitioner and (e) the date on which signed. WPS Health Insurance, the Medicare Administrative Contractor (MC) for a number of Midwestern states, provides the following example of an attestation:
The Medicare MACs provide further information on their individual websites; it may also be worthwhile to check whether your managed care payers have specific requirements. Signatures are not the proverbial rocket science, but they are critical. Any request from a MAC or other reviewer for a log or attestation should receive a speedy response so that payment is not delayed.
↧
Has Someone Gotten In Trouble For Doing That? Lessons for Anesthesia Groups from Real Cases
Anesthesia billing is complex and riddled with a minefield of potential compliance issues. Thoughtful anesthesia groups have effective compliance programs in place, designed to minimize the risk of government allegations of fraud and abuse. When crafting and maintaining an effective billing compliance program it is helpful to understand which areas of anesthesia billing have been the subject of legal action. Moreover, like it or not, when a compliance officer is able to point to specific instances in which anesthesia providers have been subject to criminal or civil penalties, s/he is more able to obtain the highest level of compliance from otherwise recalcitrant providers. This article will provide information on where to find details on legal cases impacting anesthesia providers and discuss strategies for implementing the lessons that can be learned from a thorough understanding of the cases.
How to Find the Cases
 The government understands the value of publicizing the cases it brings against providers and uses a number of venues to report on its successful legal actions. Anesthesia providers can also learn about cases of interest from their specialty societies and the media.
The government understands the value of publicizing the cases it brings against providers and uses a number of venues to report on its successful legal actions. Anesthesia providers can also learn about cases of interest from their specialty societies and the media.
The Office of Inspector General
The Office of Inspector General for the Department of Health and Human Services (OIG) was established in 1976 to fight waste, fraud and abuse in Medicare, Medicaid and more than 100 other HHS programs. Currently there are approximately 1,600 OIG employees dedicating a majority of their time to oversight of Medicare and Medicaid through a nationwide network of audits, investigations and evaluations to assist in the development of cases for criminal, civil and administrative enforcement. See http://oig.hhs.gov/about-oig/about-us/index.asp.
The OIG has an easily navigable website (http://oig.hhs.gov/) that contains information on OIG focus areas and legal actions against providers including:
- Criminal and civil enforcement actions: The OIG posts information on its criminal and civil enforcement actions often related to its work as part of the Medicare Fraud Strike Force and the Health Care Fraud Prevention and Enforcement Action Team. In addition to information on current actions there is an archive going back to 2003. See http://oig.hhs.gov/about-oig/about-us/index.asp.
- State enforcement actions: The OIG posts information on cases handled by state Medicaid Fraud Control Units that operate in 49 States and the District of Columbia. In addition to information on current actions there is an archive going back to 2010. See http://oig.hhs.gov/fraud/enforcement/state/index.asp.
- Civil monetary penalties and affirmative exclusions: The OIG posts information about providers who resolved cases in which the OIG sought civil monetary penalties, assessments and/or exclusions based on allegations of fraud and abuse. Please note that these cases are generally resolved through a settlement agreement with the provider denying liability. In addition to information on current cases there is an archive going back to 2003. See http://oig.hhs.gov/fraud/enforcement/cmp/false_claims.asp.
- Semiannual Report to Congress: The OIG issues a semiannual report to Congress keeping it informed of the OIG’s activities, significant findings and recommendations. The Semiannual Report often contains information on significant fraud and abuse cases and initiatives. In addition to the current Semiannual Report there is an archive going back to 1996. See http://oig.hhs.gov/reports-and-publications/archives/semiannual/index.asp.
In addition, the OIG publishes a Work Plan every year. Although this Work Plan does not contain specific cases, it does set forth some of the focus areas for the OIG for the current and upcoming years. Since 2013, the Work Plan has included the following anesthesia issue:
 Anesthesia services—Payments for personally performed services We will review Medicare Part B claims for personally performed anesthesia services to determine whether they were supported in accordance with Medicare requirements. We will also determine whether Medicare payments for anesthesia services reported on a claim with the “AA” service code modifier met Medicare requirements. Physicians report the appropriate anesthesia modifier code to denote whether the service was personally performed or medically directed. (CMS, Medicare Claims Processing Manual, Pub. No. 100-04, ch. 12, § 50) Reporting an incorrect service code modifier on the claim as if services were personally performed by an anesthesiologist when they were not will result in Medicare's paying a higher amount. The service code “AA” modifier is used for anesthesia services personally performed by an anesthesiologist, whereas the “QK” modifier limits payment to 50 percent of the Medicare-allowed amount for personally performed services claimed with the “AA” modifier. Payments to any service provider are precluded unless the provider has furnished the information necessary to determine the amounts due.
Anesthesia services—Payments for personally performed services We will review Medicare Part B claims for personally performed anesthesia services to determine whether they were supported in accordance with Medicare requirements. We will also determine whether Medicare payments for anesthesia services reported on a claim with the “AA” service code modifier met Medicare requirements. Physicians report the appropriate anesthesia modifier code to denote whether the service was personally performed or medically directed. (CMS, Medicare Claims Processing Manual, Pub. No. 100-04, ch. 12, § 50) Reporting an incorrect service code modifier on the claim as if services were personally performed by an anesthesiologist when they were not will result in Medicare's paying a higher amount. The service code “AA” modifier is used for anesthesia services personally performed by an anesthesiologist, whereas the “QK” modifier limits payment to 50 percent of the Medicare-allowed amount for personally performed services claimed with the “AA” modifier. Payments to any service provider are precluded unless the provider has furnished the information necessary to determine the amounts due.
See http://oig.hhs.gov/reports-and-publications/workplan/index.asp. With anesthesia in the OIG’s spotlight, it behooves practices to keep abreast of current OIG enforcement actions.
The United States Department of Justice
The Department of Justice (DOJ) is tasked with enforcing all of the laws of the United States, including everything from bank robbery to drug trafficking to terrorism. Within the mix, and as a one of its top priorities, the DOJ enforces the laws surrounding healthcare fraud and abuse. The civil and criminal prosecutions for the DOJ are handled in branch offices located in each state, with some states having multiple branch offices. See “Find Your United States Attorney” at http://www.justice.gov/usao/find-your-united-states-attorney. Importantly, each branch office has its own website, most issuing press releases (and holding press conferences) on indictments, settlements and convictions. Savvy compliance officers recognize that careful monitoring of the website for the United States Attorney’s office in their jurisdiction can lead to valuable information on those areas in healthcare under the most vigorous investigation where their practice is located.
Specialty Societies
Both the American Society of Anesthesiologists (www.asahq.org) and the American Medical Association (http://www.ama-assn.org/ama) publish information on cases involving healthcare fraud and abuse. Anesthesiologists can also visit the websites for their state societies for information specific to the states in which they practice.
Media and Social Media
As mentioned above, the DOJ issues press releases on its cases and resolutions. These press releases often lead to more in-depth reporting in traditional local and national media outlets. Not surprisingly, social media has gotten into the fray with information on healthcare fraud cases in on-line publications, blogs and even on YouTube. See, e.g., https://www.youtube.com/watch?v=WeAVD0oMoHA.
Cases and Lessons Learned
The following cases give anesthesia providers a glimpse into the areas of interest to federal and state prosecutors (both civil and criminal) relating to anesthesia practices. Each set of cases is followed by the lessons that can be learned from the cases.
ANESTHESIA TIME
Endoscopy Center of Southern Nevada – Tonya Rushing and Dr. Dipak Desai
Ms. Rushing was the CEO of the now defunct Endoscopy Center of Southern Nevada and owned the billing company that submitted claims for the Endoscopy Center. The government alleged that Ms. Rushing instructed the anesthetists employed by the Endoscopy Center to overstate their time on the anesthesia records and then she instructed the billing company staff to rely on the false anesthesia times when submitting claims. The billing company received nine percent of net collections on the fraudulently billed time for services rendered. Ms. Rushing pled guilty to conspiracy to commit healthcare fraud and was sentenced to one year and a day in prison, two years of supervised release, 150 hours community service, a $10,000 fine and $50,000 in restitution.
Dr. Dipak Desai owned the Endoscopy Center. The government alleged that Dr. Desai had the CRNAs use left-over anesthesia drugs in previously opened vials and that he used the same colonoscopy scopes and bite plates from patient to patient. More than 50,000 patients were warned to be tested for hepatitis and HIV, nine patients contracted incurable hepatitis C, and at least two patients died from the illness. Dr. Desai was found guilty of second degree murder and insurance fraud and was sentenced to life in prison with possible parole after 18 years.
The CRNAs that provided the anesthesia services and knew about the reuse of the scopes and bite plates were also charged criminally. Anesthetist Ronald Lakeman was convicted of insurance fraud and criminal neglect and sentenced to eight to 21 years in prison. Anesthetist Keith Mathahs pled to criminal neglect of patients resulting in death, insurance fraud and racketeering but was sentenced to only 28–72 months in prison because he cooperated with prosecutors and testified against the other defendants. See https://www.fbi.gov/lasvegas/press-releases/2015/endoscopy-center-ceo-sentenced-in-billing-fraud-scheme, http://www.reviewjournal.com/news/nurse-anesthetist-sentenced-prison-hepatitis-c-outbreak, http://www.reviewjournal.com/news/desai-sentenced-life-prison-possibility-parole-hepatitis-outbreak.
US v. Cabrera and Arbona
The government brought a civil case against an anesthesiologist and his billing clerk alleging overbilling of anesthesia time. Interestingly, the government investigators substantiated the allegations by comparing the billed time to the operating reports, anesthesia records and nursing notes. The defendants were found joint and severally liable for $1.3 million dollars. See http://www.leagle.com/decision/2000340106FSupp2d234_1307.xml/U.S.%20v.%20CABRERA-DIAZ.
Anesthesia time is an integral part of anesthesia billing and will always be a considered a compliance risk area. An effective compliance program should include education of providers and billing staff regarding the definition and documentation of anesthesia time along with regular audits of records with a special emphasis on comparing the anesthesia record to the facility records to ensure the accuracy of the documented anesthesia time. Groups should also consider billing directly from the anesthesia record so that the billing staff can compare the anesthesia time to the monitoring grid to confirm congruence. Finally, cases that involve poor quality of care often lead to increased interest in prosecution and enhanced penalties.
MEDICAL DIRECTION
Vanderbilt University Medical Center
This case was filed as a whistleblower lawsuit by a former anesthesiologist with the group. The allegations are that the group submitted claims for medical direction without meeting the seven steps (e.g., the anesthesiologist was in a separate building and therefore not immediately available) and that the electronic medical record provided anesthesiologists with only one choice for describing the level of treatment, “medically directed,” even though treatment of patients almost never met the necessary criteria. See https://www.nashvillepost.com/news/2013/9/11/whistleblowing_docs_allege_vast_vumc_medicare_billing_deception. This case remains pending.
Dr. Richard Toussaint
Dr. Toussaint was indicted in May 2015 on 17 counts of healthcare fraud against Blue Cross Blue Shield, UnitedHealthcare and the Federal Employees Health Benefits Program. The charges against Dr. Toussaint, an anesthesiologist and founder of a chain of upscale hospitals in Texas, are for claiming that he was present and personally participating in the anesthesia services when in fact he was under anesthesia himself or on a private jet or in another state. The indictment states that Dr. Toussaint would:
- Hand-write his initials in both the top and bottom right sections of the medical record in the ‘Pre- Anesthesia Consultation & Plan’ and ‘Anesthesia & Surgical Vents’ sections and then leave the hospital;
- Hand-write on the chart ‘Present for induction and emergence’ along with his initials—knowing he would not be present for these events; and,
- Order nurses and other caregivers to falsely claim he was present when he was not.
If convicted, Dr. Toussaint faces ten years in prison for each count of healthcare fraud and a $250,000 fine in addition to forfeiture of several luxury cars allegedly purchased with the fraudulently acquired money including a 2016 Bentley, a 2012 Rolls-Royce Ghost and a 2015 McLaren 650S Spider. See http://www.dallasnews.com/news/crime/headlines/20150520-dallas-anesthesiologist-to-plead-not-guilty-to-17-counts-of-health-care-fraud.ece, http://healthcare.dmagazine.com/2015/05/20/feds-indict-founding-physician-of-forest-park-medical-center-on-17-counts-of-healthcare-fraud/.
Lessons Learned
 With the medical direction modifiers included in the OIG Work Plan and the filing of cases involving the seven steps of medical direction, thoughtful compliance officers understand the need for effective training of anesthesiologists and billing staff on medical direction criteria and exceptions. Groups should consider billing directly from the anesthesia record (rather than a charge document) so that the billing staff can append the correct medical direction modifier based on the actual documentation in the record.
With the medical direction modifiers included in the OIG Work Plan and the filing of cases involving the seven steps of medical direction, thoughtful compliance officers understand the need for effective training of anesthesiologists and billing staff on medical direction criteria and exceptions. Groups should consider billing directly from the anesthesia record (rather than a charge document) so that the billing staff can append the correct medical direction modifier based on the actual documentation in the record.
Moreover, compliance officers should conduct regular compliance auditing of records to ensure that the correct modifier is being billed. For anesthesia groups that are using an EMR, the compliance program should include a review of the EMR to ensure that anesthesiologists have the ability to bill all level of services and are not forced to select medical direction in those instances in which the seven steps were not met.
An effective compliance program should include policies requiring providers and other employees to report any potential fraudulent conduct to the compliance officer/compliance committee so that the group can take the necessary corrective action. Failure to correct potentially fraudulent conduct can lead to a whistleblower lawsuit.
Finally, under federal law the DOJ can prosecute cases for alleged fraud involving commercial insurance companies. An effective compliance program must include substantive and procedural policies applying to commercial insurance companies including a careful review of contracts with the insurance companies and relevant state laws.
PRE-DOCUMENTING CASES
University of California – Irvine
This case was filed as a whistleblower lawsuit by a former professor/ anesthesiologist and was settled for $1.2 million. As in the Vanderbilt case, the whistleblower alleged that the anesthesiologists were not meeting the seven steps of medical direction as the physicians would be in a different building at the time they claimed to be medically directing. What distinguished this case was the fact that the government conducted an unannounced site visit and reviewed anesthesia records in which the anesthesiologist had pre-documented cases to make it appear that s/he was present including cases where the anesthesiologist had filled out the record before the case started, and cases where the record was fully documented through emergence despite the fact that the patient was still in the middle of surgery. See http://articles.latimes.com/2013/mar/28/%20local/la-me-uci-medical-20130328, http://articles.latimes.com/2008/sep/26/%20local/me-ucirvine26.
 Both the Toussaint case and the UC Irvine case focus on providers documenting anesthesia records before services were provided, which the government considers a quality of care issue as well as a potential fraud issue. Documentation of services should be done contemporaneously with the service rendered, or after the fact in an accurate and open amendment, but should never be done prior to the service rendered. Anesthesia groups should, if necessary, educate providers to ensure that they understand that records should not be pre-documented. In those instances where pre-documentation has occurred, groups should take corrective action, including disciplinary action, against the offending provider.
Both the Toussaint case and the UC Irvine case focus on providers documenting anesthesia records before services were provided, which the government considers a quality of care issue as well as a potential fraud issue. Documentation of services should be done contemporaneously with the service rendered, or after the fact in an accurate and open amendment, but should never be done prior to the service rendered. Anesthesia groups should, if necessary, educate providers to ensure that they understand that records should not be pre-documented. In those instances where pre-documentation has occurred, groups should take corrective action, including disciplinary action, against the offending provider.
Moreover, compliance officers should understand and educate providers regarding the appropriate way to amend a medical record. Medicare provides guidance on this issue at http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/Downloads/SE1237.pdf.
HEALTHCARE FRAUD AND FALSIFYING RECORDS
Dr. Paul Madison and Jeanette Shin
Dr. Paul Madison and Jeanette Shin were indicted in 2012 for alleged healthcare fraud against private insurance companies and the federal workers compensation program. If convicted, Dr. Madison faces ten years in prison and a $1.5 million fine and Ms. Shin faces six years in prison and a $750,000 fine. The allegations against Dr. Madison were that he: (1) claimed to provide anesthesia services to patients undergoing chiropractic manipulation under anesthesia (MUA) that were not performed; (2) disguised fraudulent billings by creating false medical and billing records; (3) directed billing staff, nurses, chiropractors to create false records; and (4) directed staff to lie to investigators. The allegations against Ms. Shin are that she falsified her nurse’s reports by claiming the chiropractors performed MUAs under anesthesia when she knew it was not true. This case is not yet resolved. See http://www.justice.gov/archive/.
Lessons Learned:
As with the Toussaint case, the government charges included alleged fraud against commercial insurance companies. Savvy compliance officers include policies regarding accurate documentation and billing to commercial insurance companies as an integral part of their compliance program. Compliance education and monitoring should also include close attention to commercial payers.
The government will seek redress against not only the provider that benefitted financially from the fraud, but also against office staff who did not benefit directly; it is the act of fraud and not the money directly received from the fraud that dictates government action.
DISTRACTED ANESTHESIA PROVIDERS
Milne v. Medical City Dallas, Rinkenberger (surgeon) and Spillers (anesthesiologist)
 Drs. Rinkenberger and Spillers were sued for malpractice after a patient died 10 hours after an AV node ablation. Allegations in the complaint against Dr. Spillers included “distracted doctoring.” Dr. Rinkenberger testified at his deposition that Dr. Spillers failed to notice dangerously low blood oxygen levels until 15 or 20 minutes after the patient turned blue and that he saw Dr. Spillers on a cell phone and an iPad when he should have been closely monitoring the patient. Dr. Spillers admitted that he goes on to the internet while personally providing anesthesia stating:
Drs. Rinkenberger and Spillers were sued for malpractice after a patient died 10 hours after an AV node ablation. Allegations in the complaint against Dr. Spillers included “distracted doctoring.” Dr. Rinkenberger testified at his deposition that Dr. Spillers failed to notice dangerously low blood oxygen levels until 15 or 20 minutes after the patient turned blue and that he saw Dr. Spillers on a cell phone and an iPad when he should have been closely monitoring the patient. Dr. Spillers admitted that he goes on to the internet while personally providing anesthesia stating:
“I have logged on to the Internet before especially if—specifically if I have a question about the patient's yes, we'll often, you know, do a search and find out information pertaining to the case. I will occasionally check e-mail. I will occasionally check scheduling for the office. But in general, no, I—the time spent on the Internet during a case is, you know, very brief, a couple, three minutes.”
Dr. Spillers denied that he posted on Facebook during cases when, in fact, the plaintiff ’s attorney had obtained the following postings from Dr. Spiller’s Facebook page:
- “After enduring the shittiest Friday I’ve had in a while I just found out my next patient has lice. Freakin lice. I didn’t even know they still made those. Help.”
- A picture of an anesthesia monitor with the post, “Just sitting here— sitting here watching the tube on Christmas morning. Ho ho ho.”
See http://www.dallasobserver.com/news/dallas-anesthesiologist-being-sued-over-deadly-surgery-admits-to-texting-reading-ipad-during-procedures-7134970 and https://stanfordhealthcare.org/health-care-professionals/medical-staff/medstaff-update/2013-february/201302-distracted-doctoring-and-patient-safety.html. As of the writing of this article there has been no final disposition of this malpractice action.
Lessons Learned
Aside from the fact that plaintiff attorneys are increasingly including distracted provider allegations in malpractice litigation, the use of electronics and social media while providing anesthesia has implications for the relationship between the anesthesia group, surgeons and hospital administration. Anesthesia groups are increasingly evaluated on “customer service” and the use of electronics and social media during patient care looms large as a major concern to facilities and surgeons. Prudent anesthesia groups should have a policy on the use of electronics and social media including the circumstances in which electronics can be used and the consequences for failure to comply with the policy.
Conclusion
An effective compliance program is the key to ensuring that all services are accurately and adequately documented and that all submitted claims and payments are correct. Thoughtful compliance officers review government and commercial payer resources regularly to ensure that their groups remain current on the state of the law and the claims policies of both governmental and commercial insurance programs. They also educate and monitor claims on a regular basis to assess provider compliance and take corrective action as needed to safeguard the group from fraud and abuse.
↧
Anesthesia Business Consultants Establishes ICD-10 Hotline for Their Clients
Thursday, October 1, 2015 is the date on which all providers must start using ICD-10 diagnosis codes on their claims. We cannot overstate the importance of compliance. Claims must contain a valid ICD-10 code in order to be paid.
ABC, as part of our commitment to compliance, is stepping up our efforts to help clients make a successful transition by offering an ICD-10 hotline. Beginning October 1st the ABC ICD-10 hotline, staffed by ICD-trained coders, will be available to handle your urgent questions. If you need help selecting the appropriate ICD-10 code, reporting services that span October 1st, figuring out what further information you need and where to find it, or answering any other questions regarding the new codes, we encourage you to call the ICD-10 hotline between the hours of 8:00 a.m. and 6:00 p.m. EST.
Clients will be given the number for the ICD-10 hotline by their ABC client services representative prior to October 1st. Clients are invited to listen to the ICD-10 webinar we are offering at various times between September 24th and September 30th. You may sign up to attend the webinar on our website or contact your account manager for more details.
CMS continues to offer information on its Medicare Fee-For-Service Provider Resources web page. We urge all providers to use the CMS resources as well as those provided by your professional societies.
We want to be satisfied that ABC has done everything possible to minimize delayed payments and other disruptions for our clients as we navigate this critical transition together.
↧
↧
Cadillacs in Anesthesia Practices
One feature of the Affordable Care Act (ACA) that has received limited attention is the high-cost plan tax (HCPT), aka the “Cadillac plan” tax. Beginning in 2018, employer health benefit plans with a value exceeding certain thresholds will be subject to an excise tax of 40 percent on the incremental costs of those benefits. This tax is likely to affect anesthesia practices in two ways: (1) in many instances, patients with employer-provided insurance may be responsible for a greater share of their health costs and (2) practices that offer relatively rich health benefits may themselves owe the excise tax.
In 2018, the thresholds for the tax are $10,200 for individual coverage and $27,500 for family coverage. They will increase annually based on the general rate of inflation.
The Kaiser Family Foundation (KFF) published a report on August 25, 2015 (How Many Employers Could be Affected by the Cadillac Plan Tax?) in which the authors estimate that about 16 to 26 percent of employers offering health benefits would have at least one health plan that would exceed the $10,200 HCPT self-only threshold in 2018, the first year that plans are subject to the tax. The percentage would increase to 22/30 percent in 2023 and to 36/42 percent in 2028. The lower estimates in the third column in the KFF table below are based on premiums for health coverage plus employer contributions for health savings accounts (HSAs) and health reimbursement accounts (HRAs), which the analysts assume will increase by five percent per year. The higher estimates in the right-hand column reflect the impact of flexible spending accounts (FSAs), to which employees can contribute up to $2,550 in 2015 and an estimated $2,700 in 2018, growing to $3,600 in 2028. The employees’ cost-sharing and their FSA contributions are added to the employer-paid premiums and HSA/HRA payments to determine the total value of the health benefits.

The KFF analysts did not attempt to extrapolate from self-only plans to family plans; they used only data from the former in order to make their sources of information equivalent to each other. Still, we can assume that comparable percentages of family health plans will exceed the HCPT threshold. This is particularly true because the healthcare inflation rate and the resulting insurance costs are expected to continue outrunning the general rate of inflation.
We also assume that a certain number of anesthesia and pain management practices, whose members are relatively highly compensated, will at some point find themselves among the 16 to 42 percent of employers with Cadillac plans. Like many other such employers, they may seek to reduce the value of their health benefit programs accordingly.
In order to avoid paying the 40 percent tax, employers have begun to reduce costs by redesigning the health benefits offered to employees, as predicted by several analyses published in the last few years. A May 12, 2015 Health Affairs blog post (As Employers Try To Avoid The Cadillac Tax, Treasury And The IRS Need To Act) summarized several of these analyses. A 2014 study by the National Business Group on Health showed that 42 percent of employers surveyed will increase employee cost sharing and 37 percent will reduce spousal subsidies or implement a spousal surcharge. Another survey from late 2014, this one by Aon Hewitt, found that 33 percent of employers are reducing the value of their plan designs through higher out-of-pocket costs for their employees and that 14 percent are reducing spousal eligibility or subsidies.
Other measures that employers can take to reduce costs include eliminating covered services, eliminating higher-cost health insurance options, offering benefits through a private exchange and capping or doing away with FSAs, HSAs or HRAs. Since those tax-preferred savings accounts can increase the value of an individual employee’s health benefits by several thousand dollars, they may become casualties of HCPT benefit redesign, as will some employers’ on-site medical clinics and wellness programs. According to a November 2014 report by the American Health Policy Institute, employees could see up to a $6,150 reduction in the value of their health benefits. Some employers may compensate their workforce by increasing salaries and wages, but many others will not.
Higher out-of-pocket costs for employees generally mean greater difficulties in collecting patient balances for medical practices. Anesthesia groups will need to hone the strategies used to obtain payments from patients with high deductibles such as up-front communications about fees and extended payment plans. The best answer for many groups will be to maintain relationships with their hospitals’ collection departments so that they are able to participate in patient payment programs.
With some businesses—including some anesthesia practices—already slimming down the health benefits offered to employees, the HCPT is beginning to produce its intended effects, i.e., discouraging employers from offering overly-generous benefit plans and helping to contain health care spending. As explained in the KFF article cited above,
Health benefits offered through work are not taxed like other compensation, with the result that employees may receive tax benefits worth thousands of dollars if they get their health insurance at work. Economists have long argued that providing such tax benefits without a limit encourages employers to offer more generous benefit plans than they otherwise would because employees prefer to receive additional benefits (which are not taxed) in lieu of wages (which are). Employees with generous plans use more health care because they face fewer out-of-pocket costs, and that contributes to the growth in health care costs.
Not surprisingly, efforts are underway to repeal the tax provision. Among the proponents of repeal are insurers, who benefit from selling Cadillac plans, the U.S. Chamber of Commerce, which argues that keeping the tax will present higher costs to businesses and labor unions, which have survived in large part through their ability to negotiate generous health plans. Democratic Presidential candidates Hillary Clinton, Bernie Sanders and Martin O’Malley have all joined a number of Republican legislators in calling for repeal.
The Congressional Budget Office projects that the tax will raise $87 billion in revenues between 2018 and 2025, however, helping to fund subsidies for lower-cost health plans purchased through the ACA health insurance exchanges and to provide coverage to adults under expanded Medicaid benefits. The author of an article (Few ideas on filling 'Cadillac'-sized hole if excise tax is repealed) appearing in Modern Healthcare online on October 1st noted that “About 100 economists and health policy experts of various political backgrounds signed on to a letter released Thursday that urges Congress to keep the tax without weakening or delaying it unless they implement another tax change that would curb the growth of healthcare costs.” Observers have stated that if Congress were to pass legislation eliminating the tax, a veto by President Obama would be likely. Anesthesia groups may want to prepare for changes accordingly.
↧
When Payers Ask Anesthesiologists to Refund Overpayments
The third-party medical payment system is so complicated that incorrect payments are not uncommon. Sometimes the error is in the provider’s favor. The health insurer may ask the provider—in this instance, the anesthesia practice—to refund an alleged overpayment. How should the practice handle such requests? The American Medical Association (AMA) has published an excellent Overpayment Recovery Toolkit, which we summarize in this Alert while referring readers to the 14-page Toolkit for more detailed information.
When do payers request refunds of overpayments?
Managed care contracts typically permit the payer to recover alleged overpayments by reducing or “offsetting” overpaid amounts from pending or future claims payments. The problem does not generally arise with non-contracted payers since they are apt to reimburse the patient instead of the practice.
Payers request refunds—or offset overpaid amounts against other payments to the physicians—when any of the following occur:
Duplicate payments
Another insurer is responsible (coordination of benefits problem)
Patient’s coverage has lapsed before the service is provided
Services are not covered under the patient’s plan
Lack of required authorization for the service
Payment is inconsistent with the contract or with the applicable fee schedule
Insurer considers the service not medically necessary
The above list is not exhaustive.
Actions to take upon receiving notice of an overpayment
The first order of business is to make sure to respond within any time limits provided in managed care contract. Simply responding quickly, i.e., within a week or two, may be easier than verifying the deadline, if this is not stated in the request or notice.
According to the AMA, the first step is to review the request from the payer, whether on paper or electronic to identify the reason(s) for the request. If the request does not contain enough information to understand the alleged error or to determine the validity of the claim (a frequent occurrence), anesthesia practices should contact the payer for the necessary data, which would include applicable claim and subscriber numbers, the payer-specific alpha or numeric code to identify the overpayment recovery request; the specific amount of overpayment and how it was made to the physician, and “if the payer intends to initiate a retroactive denial on a previously paid claim to recover the overpayment, identif[ication of] the pending claims from which the payer intends to recoup or offset the overpayment or state that the recoupment or offset will be made from future claims,” and the address for payment or a telephone number, weblink or mailing address where the physician may file a dispute.
If the request for recovery of an overpayment is valid, the practice should send the payer a refund or approve recoupment from the next payment within the time limit on the notification. The AMA recommends calling the payer to alert them to the remittance if the refund is being sent within 30 or 40 days of the deadline.
It may be worth the trouble of reworking overpaid claims if the patient is responsible for payment and can be billed, or if it appears that another insurer is responsible because of a coordination of benefits mistake. In the latter case, the practice should send the claim to the secondary payer.
The request may not be valid if it is made outside the timeframe established by statute in many states. Because of the disruptive nature and effects of requests for overpayments made years ago, at least half of the states have adopted overpayment laws or regulations protecting providers by requiring that payers’ recoupment requests be made within 6, 12, 18, 24, or in one case (Florida), 30 months of the claim’s payment dates. Most of these statutes or administrative rules also exempt overpayments based on provider fraud from the time limits. It is important to be familiar with both the statutory/regulatory provisions and the timelines and other requirements spelled out in the practice’s managed care contracts. AMA members have access to a database containing “all state laws and regulations governing overpayments, as well as an issue brief, which is designed to help physicians negotiate overpayment provisions in managed care contracts and analyze the legitimacy of overpayment demands.” Non-AMA members should be able to obtain their state rules through their state medical associations or even their hospitals.
If the practice determines that the request for recovery of an overpayment is not valid, it should appeal, following the process described in the payer contract and using any prescribed forms. The practice should also submit a letter with a full explanation of the grounds for the appeal and any supporting documentation, e.g., copy of patient’s eligibility verification with dates of coverage, clinical documentation, remittance advices and explanations of benefits from all payers involved, claim submission reports for timely filing, guidelines and/or policies from the payer, etc. The AMA Toolkit suggests addressing the appeal letter to a specific person to facilitate tracking the progress of the appeal, and also inquiring about the expected time frame for processing the appeal.
In either case, whether the claim is valid and the refund is made or approved or whether it is not appropriate and is appealed, the practice should carefully notate the patient’s account and should track the information regarding the claim in order to follow up and to identify trends.
Responding to requests for overpayment refunds can consume a great deal of time and effort in an anesthesia or pain practice. In order to reduce the number of claims that result in such requests, the toolkit advises physicians “to identify the most common reasons for overpayment recovery requests and perform a deep dive into their internal processes to determine why each request occurred” and also “to perform a routine examination of your claims denial history or claims that have resulted in repeated overpayments and identify and correct the most frequent sources of those denials or overpayments.”
We hope that we have pointed readers toward a helpful reference and that fewer requests for overpayment refunds will be the result.
↧
Telemedicine Is in Anesthesiologists’ Future
Telemedicine, in one form or another, is going to be part of most physician practices within the next decade. For many doctors, it will arrive sooner, if it is not already here. Five years ago, Dr. Girish Joshi wrote in the ASA Newsletter (Global Patient Perioperative Care through Clinical Pathways, ASA Newsletter. 2010; 74(8):10-12):
Telemedicine is a term used to describe health care provided by a practitioner at a remote location with the help of advanced technologies. Telemedicine is expected to play an increasingly important role in outpatient settings (e.g., home health care, remote patient monitoring, chronic disease management and rural health care) as well as in hospital settings (e.g., emergency department and ICU). Other applications of telemedicine include battlefield medicine, maritime medicine and aviation health care. Telemedicine provided in the critical care setting is commonly referred to as e-ICU. e-ICU has been proposed as a potential means of bringing the expertise of critical care specialists to hospitals with inadequate access to intensivists. … The practice of telemedicine may also be applicable to anesthesiology in which an anesthesiologist stationed in a room (within the operating area) could monitor multiple operating rooms. The telemedicine concept combined with automated anesthesia systems or closed-loop systems may further improve patient safety.
The tools and the practice of telemedicine (for which the word “telehealth” is used interchangeably) have without doubt advanced in the last few years and even since we broached the topic in our January 13, 2014 Alert. Among the most recent developments, Mercy Health in St. Louis, Missouri has just opened a $54 million Virtual Care Center from which 290 nurses and other clinicians monitor 2,431 patient beds in 34 hospitals across five states. Have clinical practice laws and regulations and payment policy kept up? Not to the extent advocated by the proponents of telemedicine.
Professional licensure portability and practice standards
Practicing across state lines raises issues in telemedicine as in other contexts. Most, if not all, states require that a physician be licensed in the state where the patient is located, a serious impediment to telemedicine across many geographic areas.
Physician licensure requirements and procedures vary considerably between state medical boards. At one extreme, the authorities require full, unrestricted state licensure without exception in order to provide medical care whether by telehealth or any other means. According to the American Telemedicine Association’s (ATA) State Telemedicine Gaps Analysis Physician Practice Standards & Licensure report, only four states are this limiting: Michigan, North and South Dakota and Pennsylvania. (The ATA is careful to note that their reports do not constitute legal advice, a caveat that we echo. For a full understanding of law and rules applicable in their individual states, readers should consult counsel.) Other states recognize exceptions to the state-licensure requirements that ATA broadly categorizes as:
- reciprocity for bordering states (D.C., Maryland, New York and Virginia),
- physician-to-physician (P2P) consultation exemptions (e.g., Massachusetts), and
- conditional/telemedicine licenses (Alabama, Louisiana, Minnesota, Nevada, New Mexico, Ohio, Oregon, Tennessee and Texas).
No state achieved a top score on licensure portability, meaning that “every state imposes a policy that makes practicing medicine across state lines difficult regardless of whether or not telemedicine is used.” Other indicators on which the ATA measured states’ acceptance of telemedicine include:
- requiring an in-person visit before, during or after telemedicine encounters,
- adopting practice standards with higher specifications for telemedicine than for face-to-face care,
- requiring a telepresenter or health care provider on the premises during a telemedicine encounter, and
- requiring informed consent (written, verbal or unspecified) before a telemedicine encounter.
Overall, twenty-two states averaged the highest “composite grade” suggesting a supportive policy landscape that accommodates telemedicine adoption and usage. Twenty-six states and D.C. were in the middle with room for improvement. Two states (Alabama and Texas) averaged the lowest composite score, indicating many barriers for telemedicine advancement.
This is an area that is changing very rapidly. In 2015, more than 100 bills relating to telemedicine have been introduced in 36 states. Only ten of these bills would expand licensure requirements to encompass telemedicine. Arkansas is one of states that adopted a very restrictive law this year, but in September, the Arkansas State Medical Board’s Telemedicine Advisory Committee indicated that it was drafting a rule to allow establishment of a physician-patient relationship through the use of real-time audiovisual communication rather than an in-person visit, evidently seeking a way around the new statute.
Payment for telemedicine services
Twenty-three states, as well as D.C., have adopted full parity statutes requiring that private insurers pay for telemedicine services at the same or comparable rates and terms as face-to-face services. This number has doubled in the last three years alone. Maine, New Hampshire, New Mexico, Tennessee and Virginia and D.C. are ranked as the most supportive jurisdictions. Arizona is unique in having enacted a partial parity law that mandates coverage and reimbursement, but limits coverage to a certain geographic area (e.g., rural) or a predefined list of health care services. Some states with parity laws were rated lower than others in the ATA’s State Telemedicine Gaps Analysis-Coverage & Reimbursement report because of restrictions on the type of technologies (e.g., audio-visual only), services and/or conditions covered.
Many insurers even in states that do not have parity laws are voluntarily increasing coverage of telemedicine. Blue Cross and Blue Shield plans have been leaders in the field. Aetna and Cigna also provide coverage. There are other private payers, however, that continue to deny payment for telemedicine services. Physicians seeking to change their managed care organizations’ policies are advised to “communicate to MCOs that telemedicine services are part of their customary and usual practice” with letters stating their “intention to use telemedicine in the normal course of business, including notification of future claim submittal, and encourag[ing] the private payer to ask questions and make comments.” They should also add “telemedicine” to the list of covered services identified in their provider agreements and add coverage for telemedicine services to the services and obligations section of those agreements. See Telemedicine Services: Steps for Providers Seeking Reimbursement, an e-alert from the Milwaukee law firm of Reinhart Boerner Van Deuren S.C.
Twenty-four states provide some coverage for telemedicine under their state employee health plans with 21 states extending coverage under their parity laws. Medicaid is even more of a hodge-podge, as reported by the ATA, with 48 state Medicaid agencies allowing some type of coverage for services provided via telemedicine. Requirements that the patient be located at a specific type of “originating site,” such as a hospital, a doctor’s office, a federally qualified health center or a health department facility, but not their home or place of work or school, hamper the full use of telemedicine’s potential in about half of the states. Most of the states in which Medicaid covers some telemedicine services also restrict the type of provider for whom payment will be made. Florida, Idaho, Iowa and Montana ranked the lowest with coverage for physicians only.
Medicare is lagging behind. The fee-for-service program has tightly limited payments to certain rural areas and certain services because of Congress’ concern that telemedicine might increase Medicare expenses, according to a Kaiser Health News article published on June 23, 2015 (Medicare Slow To Adopt Telemedicine Due To Cost Concerns). Thus Medicare only covers a short list of services provided via telemedicine (inpatient and office visits, some behavioral and substance abuse services, transitional care management, kidney disease and diabetes care training). The originating site, i.e., the location of the Medicare beneficiary, must be (a) a rural Health Professional Shortage Area (HPSA) located either outside of a Metropolitan Statistical Area (MSA) or in a rural census tract, or (b) a county outside of a MSA. The distant site practitioners can only be physicians, nurse practitioners, physician assistants, nurse midwives, clinical nurse specialists, certified registered nurse anesthetists, clinical psychologists and social workers for non-medical services and registered dietitians or nutritionists. Finally, only the use of interactive audio and video telecommunications systems that permit real-time communication is covered. Asynchronous “store and forward” technology is permitted only in Federal telemedicine demonstration programs conducted in Alaska or Hawaii.
Although Medicare Advantage plans are beginning to offer telemedicine services, as are some Medicare accountable care organizations, fewer than one percent of Medicare beneficiaries have used the available videoconferencing technology.
Legislation has been introduced in Congress that would liberalize the rules on Medicare payment for telemedicine. The Tele-Med Act of 2015 (S. 1778/H.R. 3081), for one would allow beneficiaries to receive care from a U.S. health professional licensed by any state. The bill was referred to committee in July and is still awaiting action.
With or without Congressional action, however, telemedicine is a highly dynamic field and there is significant support for its expansion through favorable laws and regulations. Clinical applications in anesthesiology critical care and other medical specialties—and certainly primary care—will become increasingly important as value-based purchasing becomes the norm. Dr. Joshi noted five years ago that the tools of telemedicine could allow a single anesthesiologist stationed within the operating area to monitor multiple rooms. Since then, the development of software such as AlertWatch, which integrates various sources of medical data into a single dashboard view of the patient, has expanded the horizons for remote patient monitoring. In the preoperative area, pre-anesthesia assessments and consultations via telemedicine (e.g., TelePREOP) can permit the timely completion of patient evaluation and reduce the number of case cancellations on the day of surgery. Tele-technology will allow anesthesiologists to assume greater responsibilities for overseeing the post-discharge care of surgical patients. We hope that the legal and payment policy framework for these developments will advance quickly.
↧
A Basic Primer on the Bundled Payments for Care Improvement Initiative
The Centers for Medicare and Medicaid Services (CMS) Bundled Payments for Care Improvement (BPCI) initiative is comprised of four broadly defined models of care, which link payments for the multiple services beneficiaries receive during an episode of care. Under the initiative, organizations enter into payment arrangements that include financial and performance accountability for episodes of care. The intent is for these models to lead to higher quality and more coordinated care at a lower cost to Medicare.
Traditional Medicare reimburses physicians on a fee-for-service (FFS) system, through Part B, and hospitals under an inpatient prospective payment system (IPPS) through Part A. Both systems are triggered by individual services being provided to beneficiaries for a discrete illness or course of treatment. Various studies have demonstrated that this approach can result in fragmented care with minimal coordination across providers and healthcare settings. As we have heard many times, the payment systems are geared to reward the quantity of services offered by providers rather than the quality of care furnished.
The Affordable Care Act (ACA) established an Innovation Center within CMS to test alternative payment and service delivery models that have the potential to reduce health care expenditures while preserving or enhancing the quality of care. The BPCI initiative is one of a dozen initiatives that the Innovation Center is currently testing. BPCI is composed of four broadly defined care models, which bundle payments for multiple services beneficiaries receive during an episode of care. Under the initiative, organizations enter into payment arrangements that include financial and performance accountability for an entire episode. Table 1 shows the four models that a participating organization may use to develop their program.
In Model 1 in the table, the episode of care is defined as the inpatient stay in the acute care hospital. Medicare pays the hospital a discounted amount based on the payment rates established under the IPPS used in the original Medicare program. Medicare continues to pay physicians separately for their services under the FFS. Model 1 began in April 2013.
Models 2 and Model 3 involve a retrospective bundled payment arrangement where actual expenditures are reconciled against a target price for an episode of care. In Model 2, the episode includes the inpatient stay in an acute care hospital plus the post-acute care and all related services up to 90 days after hospital discharge. In Model 3, the episode of care is triggered by an acute care hospital stay but begins at initiation of post-acute care services with a skilled nursing facility, inpatient rehabilitation facility, long-term care hospital or home health agency. Under these retrospective payment models, Medicare continues to make FFS payments; the total expenditures for the episode is later reconciled against a bundled payment amount (the target price) determined by CMS. A payment or recoupment amount is then made by Medicare reflecting the aggregate expenditures compared to the target price.

In Model 4, CMS makes a single, prospectively determined bundled payment to the hospital that encompasses all services furnished by the hospital, physicians, and other practitioners during the episode of care, which lasts the entire inpatient stay. Physicians and other practitioners submit “no-pay” claims to Medicare and are paid by the hospital out of the bundled payment. Models 2, 3 and 4 began in October 2013.
CMS has developed some unique definitions for the BPCI initiative. They are:
- Awardees are entities that assume financial liability for the clinical episode spending and have signed an Agreement with CMS.
- Episode Initiators are healthcare providers that trigger BPCI episodes of care; they do not bear risk directly (unless they also serve as an Awardee), but participate in the model through an agreement with a BPCI Awardee.
- Conveners are entities that bring together multiple health care providers. These conveners can participate as either Awardees that enter into Agreements with CMS and bear risk or Facilitator Conveners that do not enter into an Agreement with CMS and do not bear risk.
Over the course of the initiative, CMS will work with the Awardees to assess whether the models being tested result in improved patient care and lower Medicare costs. Awardee Agreements may also include proposals for gainsharing among provider partners. A potential downside to the Awardee’s ability to control cost is due to beneficiaries retaining full freedom of choice to choose services and providers, including care from providers not participating in the BPCI initiative. Additionally, BPCI participants and their partnering providers are required to provide beneficiaries with written notification that explains the existence and purpose of BPCI, the beneficiary’s right of access to medically necessary services, and the beneficiary’s right to choose any provider or supplier of items or services.1
In August 2015, CMS announced that 360 organizations have entered into agreements to participate in the BPCI initiative and an additional 1,755 providers have partnered with those organizations. In addition, CMS announced a new Medicare Part A and B payment model, the Comprehensive Care for Joint Replacement Model (CCJR). (See ABC Alert A Role for Anesthesiologists in CMS’s New Comprehensive Care for Joint Replacement Payment Program, August 24, 2015.) Although the Comprehensive Care for Joint Replacement Model is distinct from the Bundled Payments for Care Improvement initiative, both initiatives are part of the innovative framework established by the ACA to move the healthcare system toward one that rewards providers based on the quality, not quantity, of care they deliver to patients.2
 Although CMS is within their mandate to establish or expand payment initiatives, BPCI results are far from conclusive. In a May 12, 2015 letter to CMS, the Healthcare Financial Management Association (HFMA) commented that BPCI models still have significant design and operational issues that should be resolved prior to any mandatory expansion.3 Also, based on CMS data, Model 2 is the only model that has seen acceptable participation. CMS’ announcement of the CCJR model is easily understood based on an examination of CMS data as of April 2015 that showed the most prevalent episode included in BPCI Models 2-4 is major joint replacement of the lower extremity.4
Although CMS is within their mandate to establish or expand payment initiatives, BPCI results are far from conclusive. In a May 12, 2015 letter to CMS, the Healthcare Financial Management Association (HFMA) commented that BPCI models still have significant design and operational issues that should be resolved prior to any mandatory expansion.3 Also, based on CMS data, Model 2 is the only model that has seen acceptable participation. CMS’ announcement of the CCJR model is easily understood based on an examination of CMS data as of April 2015 that showed the most prevalent episode included in BPCI Models 2-4 is major joint replacement of the lower extremity.4
The data to date does not suggest what type of bundled payment model CMS may endorse or mandate in the future. The timing of such a decision is likewise unknown. CMS’ aggressive goal to have 30 percent of Medicare payments in alternative payment models such as accountable care organizations and bundled payments by the end of 2016 and 50 percent in by the end of 2018,5 however, means that bundled payment initiatives and other innovation programs are here to stay in one form or another.
1 http://innovation.cms.gov/initiatives/bundled-payments/
3 “HFMA Comments on Bundled Payments for Care Improvement Initiative,” May 12, 2015. http://www.hfma.
4 CMS Innovation June 22, 2015 presentation to HFMA Patient Care Models Group.
↧
↧
The Anesthesia Conversion Factor and PQRS Changes in the Final Medicare Fee Schedule Rule for 2016
The national average Medicare anesthesia conversion factor (CF) effective January 1, 2016 will be $22.4426, down from $22.6093 in 2015, which is a decrease of $0.1667 per anesthesia unit. Geographically-adjusted CFs for the 90-odd Medicare localities are not yet available.
The general Medicare physician fee schedule CF, which is used to calculate payments for visit services and pain medicine and other non-anesthesia procedures, will be $35.8279, a decrease of 10.56 cents per relative value unit (RVU). CMS announced the new CFs in the Final Rule containing Revisions to Payment Policies under the Physician Fee Schedule and Other Revisions to Part B for CY 2016, released on October 30.
After the elimination of the Sustainable Growth Rate (SGR) formula in last spring’s Medicare Access and CHIP Reauthorization Act of 2015 (MACRA), we had hoped to see the last of the “negative updates” or cuts in Medicare payment rates. MACRA replaced the SGR with a 0.5 percent increase in the CFs each year until 2019. In the Final Rule, however, after applying the 0.5 percent update, CMS adjusted the CFs downward by 0.02 percent for budget neutrality and by a new 0.77 percent “target recapture amount.” The target recapture is an artifact of 2014 legislation that set a target reduction for adjustments for allegedly misvalued codes in each of the next three years. The target for 2016 is 1.0 percent of spending on physician services. CMS identified 0.23 percent worth of specific misvalued procedures and the balance will come from the 0.77 percent across-the-board reductions.
The anesthesia CF came in for an additional 0.445 percent reduction reflecting changes to the valuation of practice expenses and malpractice insurance costs. In assessing practice expenses, CMS applied a time adjustment of 33 percent for medical direction of two to four cases to avoid overstating the amount of time spent by the anesthesiologists involved in concurrent services.
Other changes announced in the Final Rule of significance to anesthesiologists include a reduction in the number of available PQRS measures to 281. The measures eliminated include #193, Perioperative Temperature Management. Measure #44, Preoperative Beta-Blocker in Patients with Isolated CABG Surgery, will be reportable only through a registry in 2016. The elimination of the claims-based reporting option for most anesthesia measures is going to present a challenge for many anesthesia groups. As then-ASA President J.P. Abenstein, M.S.E.E., M.D. wrote in his letter of September 8, 2015, containing ASA’s comments on the proposed fee schedule rule:
We are apprehensive that should all proposals for measures be finalized as proposed, anesthesiologists reporting via claims would have just one measure to report–PQRS #76: Prevention of Central Line Catheter (CVC)-Related Bloodstream Infections. Such a scenario would make measure reporting for many of our practices impractical.
There are five new measures that can be reported by anesthesiologists—but only using a registry-based method of reporting, despite ASA’s and others’ urging that claims-based reporting remain an option.
The new PQRS measures include #424, a revised Perioperative Temperature Management measure that requires recording of at least one body temperature greater than or equal to 35.5 degrees Celsius (or 95.9 degrees Fahrenheit) within the 30 minutes immediately before or the 15 minutes immediately after anesthesia end time. The four other new measures, all of which are already used in the Anesthesia Quality Institute’s National Anesthesia Clinical Outcomes Registry Qualified Clinical Data Registry (QCDR), like #424, are:
- Measure # 404: Anesthesiology Smoking Abstinence;
- Measure # 426: Post-Anesthetic Transfer of Care Measure: Procedure Room to a Post Anesthesia Care Unit (PACU) (using a checklist or protocol);
- Measure # 427: Post-Anesthetic Transfer of Care: Use of Checklist or Protocol for Direct Transfer of Care from Procedure Room to Intensive Care Unit (ICU), and
- Measure # 430: Prevention of Post-Operative Nausea and Vomiting (PONV) – Combination Therapy.
CMS is adding a reporting option that will allow group practices to report quality measure data using a QCDR. This option should be helpful to groups (consisting of two or more eligible professionals) that choose the QCDR option since their performance will be analyzed at the group level, i.e., CMS will examine whether a sufficient number of measures and domains were reported for 50 percent of the group’s patients rather than for 50 percent of the individual physician’s patients.
One of a number of other provisions in the Final Rule that will also be of interest to anesthesiologists involve the procedures that CMS believes to be potentially misvalued and that the AMA/Specialty Society Relative Value Update Committee will be asked to review. These procedures include anesthesia for upper and lower gastrointestinal endoscopy, emergency intubation and insertion of central venous and arterial catheters. Any modifications will be implemented after next year’s rulemaking cycle.
We will provide more information on the PQRS changes and on other critical matters in the Final Rule, in upcoming blogs.
↧
Anesthesia Informatics: The Future is Upon Us
Anesthesia practice management used to be relatively simple. Bill correctly, collect aggressively, and everyone is happy. It is true that Medicare and managed care made getting paid a little more challenging, but a good day’s work in most facilities generally resulted in enough revenue to cover the cost of the providers, and when it didn’t most hospitals have been willing to make up the difference with some level of stipend or revenue guarantee.
Most anesthesia providers would argue that for all the payment challenges created by diverse payer rules, fee for service medicine is still the preferred system. They like the fact that you get paid to provide services. What they don’t like are the increasing layers of complexity being imposed by efforts to measure quality and appropriateness of care. Especially concerning is the perception that what started as a trickle of inconvenient reporting requirements is gaining momentum to form a river of change that threatens to wash away any vestige of the once familiar mode of practice. Many older doctors are glad their time as anesthesiologists is almost up. They understand that it will be up to the next generation to find opportunity in what appears to be an irreconcilable sea of constraints and regulations.
The Good Old Days
 Remember the days of 4-by-6-inch charge books that fit in the pocket of hospital greens? Anesthesia providers got quite good at documenting what they could bill to patients and their insurance. There was never a doubt about the surgical procedure, the start and end times of cases or any of those unusual patient or operative factors that might apply. Their charge tickets even included little check boxes for the other services they might be able to include such as invasive monitoring, transesophageal echocardiography, the administration of nerve blocks for post-operative pain management and ultrasonic guidance. There was a certain freedom that was consistent with the history and culture of the specialty. Each provider developed his or her own protocols and approaches and billed accordingly. Anesthesia has always prided itself on its autonomy. Such notions as peer review, provider profiling or performance assessment were just not a major part of the culture of the specialty. I can remember asking an anesthesiologist if anesthesia were art or science and he said yes!
Remember the days of 4-by-6-inch charge books that fit in the pocket of hospital greens? Anesthesia providers got quite good at documenting what they could bill to patients and their insurance. There was never a doubt about the surgical procedure, the start and end times of cases or any of those unusual patient or operative factors that might apply. Their charge tickets even included little check boxes for the other services they might be able to include such as invasive monitoring, transesophageal echocardiography, the administration of nerve blocks for post-operative pain management and ultrasonic guidance. There was a certain freedom that was consistent with the history and culture of the specialty. Each provider developed his or her own protocols and approaches and billed accordingly. Anesthesia has always prided itself on its autonomy. Such notions as peer review, provider profiling or performance assessment were just not a major part of the culture of the specialty. I can remember asking an anesthesiologist if anesthesia were art or science and he said yes!
For years anesthesia has operated in the shadows, an arcane world whose true value was really only understood by its practitioners. “Who is that masked man?” was the title of a Newsday feature article about Dr. Peter Walker, a Long Island anesthesiologist, in 1982. Those were the days when anesthesia was a free good for hospitals, meaning it did not cost the hospital anything to contract with a group for professional services. Then everything started to change. Payers started to question the cost of anesthesia care and hospitals started to get insistent requests for financial support from their contracted anesthesia providers. As the economics of care started to change customers and payers started asking questions. Ultimately the specialty ended up under the magnifying glass.
 The evidence of this change has been both general and specific. In general terms the overall cost of American healthcare has become a topic of public debate and anesthesia is no exception. The impact of this transition has been especially evident in payer contract negotiations. But specifically with regard to the specialty, as each individual anesthesia practice made its case for some level of financial support to hospital administration more questions were being raised about what they were getting for what they were paying. This has proved to be a rude awakening for many anesthesia practices. The specialty was crossing over from a world in which providers got paid for what they billed to one in which they got paid for what they negotiated.
The evidence of this change has been both general and specific. In general terms the overall cost of American healthcare has become a topic of public debate and anesthesia is no exception. The impact of this transition has been especially evident in payer contract negotiations. But specifically with regard to the specialty, as each individual anesthesia practice made its case for some level of financial support to hospital administration more questions were being raised about what they were getting for what they were paying. This has proved to be a rude awakening for many anesthesia practices. The specialty was crossing over from a world in which providers got paid for what they billed to one in which they got paid for what they negotiated.
PQRS
So what? Was anything really changing in the life of the typical anesthesia provider? Yes and no. The first incursion was the Centers for Medicare and Medicaid Services (CMS’) Physician Quality Reporting System (PQRS). What a curious phenomenon! The intent was to implement some quality measures specific to anesthesia, yet the result was a set of process measures:
- Administration of antibiotic within an hour before incision
- Use of sterile technique for central venous catheter placements
- Use of active temperature management for cases 60 minutes or longer
The original list of PQRS official measures started to grow and morph. Anesthesia providers did too well with the documentation of antibiotics so the administration of beta-blockers was added to the list and ultimately antibiotic prophylaxis came off. Each year there was a new iteration. What started as a small bonus evolved, as planned, into a potential penalty for non-compliance.
One might argue that the most curious of these is the recent PQRS “crosscutting” measure #47, which will probably be short-lived. Anesthesia providers who round on patients with continuous catheters—like doctors performing primary care visits in their offices—are expected to ask the patients if they have an advance care directive. They don’t have to look at it or know what is included. They simply need to document that they asked about it and what the answer was. While there is actually some quite compelling literature, justifying how such a measure applies to anesthesia is a little mystifying. Fortunately, most anesthesiologists will not be affected, but even so this is a preview of coming attractions.
Meaningful Use
Meaningful use was another curious experiment in physician behavior modification. Providers started receiving bonus payments to capture information that potentially could be used to populate a patient healthcare portal. Many of us wondered about such rich incentives for a program that appeared to have such limited potential benefits. Now the incentives to implement electronic medical records are considerably more complex.
Little by little, though, a pattern is emerging here. It is not hard to see where this is taking American medicine. The simple mechanics of fee-for-service medicine are giving way to an entirely new era of healthcare informatics. While a pen, an anesthesia record and a good billing agent used to be the essential keys to financial success, a whole new set of high-tech tools is becoming necessary to keep abreast of the rapidly changing face of healthcare informatics.
ICD -10
What should we make of the transition from ICD-9-CM to ICD- 10-CM diagnosis coding, which must be completed by October 1, 2015? Is it the big deal that many practices are worried about, or will it prove to be another of those transitions where the advanced hype outstripped the reality of implementation?
It is a big deal and its implementation will further justify the argument for a perioperative surgical home.
Essentially, an inconspicuous formalistic element of the claim process that never had anything to do with the justification of the anesthetic will become a critical piece of information for payment of the anesthesia claim. This is no small thing. Not only are the logic and structure of ICD-10 codes considerably more complex and intricate that the previous coding sequence, but now there is an expectation that everyone in the operating room who participates in the care of the patient should know why this patient is having this procedure at this point in time. Payers will actually have the ability to use the information on the anesthesia claim to validate the surgical claim, the consequences of which could dramatically impact denials and cash flow.
Figure 1 is a typical ICD-10 decision tree for colonoscopy services. It highlights the logic of the new sequence. While the typical anesthesia diagnosis for a polypectomy might have been limited to “polyp(s),” such a shorthand summary will not be sufficient after October 1st for a qualified ICD-10 coder to determine an appropriate and valid ICD-10 code, the absence of which would surely increase the risk that the claim would be denied by the payer. In order to avoid significant increases in denials and the resulting impact on cash flow, anesthesia providers are having to step up to the plate to master a new language and change how they document the diagnostic justification for the surgical procedure performed.

Table 1 presents a list of valid coding options for a typical colonoscopy. The anesthesia provider must provide sufficient detail in the diagnosis so that a qualified ICD-10 coder can make an appropriate determination. The real question, of course, is whether the endoscopist can make the determination.
Anyone who thinks the transition will go smoothly has not taken the time to look into the details. The logic and the level of detail required vary greatly from one surgical procedure to another. The good news is that about 25 common procedures account for 60 percent of all surgical cases so the list of frequently performed procedures with which anesthesiologists must become familiar is fairly short.
There is a curious irony at work here. If the intent of ICD-10 is to give the payer a means of validating the surgeon’s diagnosis, then it is a very imperfect method. How do payers think the anesthesia provider will confirm the details of the post-operative diagnosis if not by means of a post-operative time out? Actually, it is starting to appear as if many anesthesia providers are better prepared than their surgical colleagues, thanks in no small measure to the full court press put on by ABC to educate all its clients.
 What could possibly justify such a disruption? Proponents such as the American Healthcare Information Management Association (AHIMA) argue the new codes could greatly improve our ability to:
What could possibly justify such a disruption? Proponents such as the American Healthcare Information Management Association (AHIMA) argue the new codes could greatly improve our ability to:
- Modernize and expand capacity to keep pace with changes in medical practice and healthcare delivery by providing higher quality information for measuring service quality, outcomes, safety and efficiency;
- Enable better patient care through better understanding of the value of new procedures, improved disease management, and improved ability to study and understand patient outcomes;
- Improve data capture and analytics of public health surveillance and reporting, national quality reporting, research, and data analysis, and provide detailed data to inform healthcare delivery and health policy decisions.
Like it or not, one of the greatest shortcomings of the current healthcare delivery system is its lack of coordination among providers, which is one of the underlying motivations for the implementation of electronic medical records (EMRs). Individual providers, and this is especially true of most anesthesia practices, tend to operate independently and in a vacuum. Such atomistic behavior and isolated charting practices are certainly not conducive to a detailed analysis of patterns of care that could result in process improvement.
The point is there is no turning back. Academicians, clinical researchers and politicians are insisting on answers to complex and detailed questions about the nature of healthcare utilization and cost. There is a broad-based commitment to finding ways to better manage quality and cost. Anesthesia providers have no choice but to embrace the logic of ICD- 10 and find ways to collaborate with their surgical colleagues in the post-operative determination of appropriate diagnoses.
While the implementation of ICD-10 will preoccupy most providers for the balance of 2015 and into 2016, there is yet another challenge looming ahead of us. CMS is committed to move from the cumbersome claims-based reporting of PQRS indicators to registry reporting. Again this is one of these ideas that make sense if you take a long-lens view, but it is being perceived as just one more complicating factor in the delivery of compassionate and quality healthcare.
Where and how will it all end? At what point does the provision of care become less relevant than the documentation of the care? It is almost Kafkaesque especially when we consider what is being contemplated as the next step in the unfolding saga of clinical documentation requirements: the Qualified Clinical Data Registry (QCDR) (and the Anesthesia Quality Institute’s [AQI] QCDR is arguably the most important such registry for anesthesia).
QCDR
 If you want a simple way of thinking about the QCDR try this: Make a list of all the various aspects of anesthesia care that could be measured and which might tell us something about the quality of the care provided. Put them all together and you have a rough approximation of the basic vision for the QCDR. The AQI’s proposed list for its QCDR currently includes 41 measures.
If you want a simple way of thinking about the QCDR try this: Make a list of all the various aspects of anesthesia care that could be measured and which might tell us something about the quality of the care provided. Put them all together and you have a rough approximation of the basic vision for the QCDR. The AQI’s proposed list for its QCDR currently includes 41 measures.
The proposed plan is that each practice will pick nine measures to report. The measures are grouped into the following domains of which three must be represented by the measures selected.
- Person and Caregiver-Centered Experience
- Patient Safety
- Communication and Care Coordination
- Community and Population Health
- Effective Clinical Care
The measures are further grouped into process and outcomes measures. “Measure #6: PACU Transfer of care: use of checklist” would represent a process measure. “Measure #11: Immediate perioperative cardiac arrest rate” would be considered an outcomes measure. Each practice must report at least two outcomes measures.
 The good news is that the proposed plan allows for considerable flexibility in choosing measures that appear reasonable and relevant to the practice. The challenges will be the practical considerations associated with data capture and reporting. Those with EMRs will find such data capture relatively easy while those still using paper forms will have to modify their forms or add a new form.
The good news is that the proposed plan allows for considerable flexibility in choosing measures that appear reasonable and relevant to the practice. The challenges will be the practical considerations associated with data capture and reporting. Those with EMRs will find such data capture relatively easy while those still using paper forms will have to modify their forms or add a new form.
The other aspect of QCDR reporting that cannot be overlooked is that this will represent a change in submission methodology. Currently PQRS measures are included on Medicare claims as CPT codes. The plan is to migrate to a registry-based reporting system whereby the measures are sent to CMS. This will impose yet another layer of connectivity on each practice. There are various registry options open to anesthesia practice but most will probably choose the AQI QCDR. It is too early to tell what the full impact of this transition will be but this project will no doubt occupy most practices next year.
Challenge and Opportunity
It has always been one of the great ironies of anesthesia that despite the dazzling array of space-aged technology used in the operating room to manage patients safely through all manner of clinical obstacles and complications, anesthesia record-keeping still tends to be rather byzantine. Clearly, this is changing rapidly. The historical reporting tools simply cannot support the data requirements of tomorrow’s medicine.
In her book Confidence: How Winning Streaks and Losing Streaks Begin and End, Harvard Business School professor Rosabeth Moss Kanter identifies three qualities that consistently distinguish organizations that evoke confidence in their customers and employees. They are:
- Accountability
- Collaboration
- Innovation
It is becoming quite clear that these are the very qualities that the American public is seeking in our current healthcare system. While the various developments described above may appear to physicians as part of a vast conspiracy arraying itself against organized medicine these are simply attempts, imperfect and inchoate as they are, to bring some order to the chaos and inconsistency of the present system. There needs to be a realignment of incentives such that the system works more as a whole rather than as a collection of individual practices.
So where, you may be wondering, is there any opportunity to profit or gain from such a complicated overlay of reporting requirements? Sometimes one player’s advantage comes at the expense of another’s failure. It is true that the focus of all these developments is analytics, but the ultimate objective is far more significant. Either your practice is making the necessary investment in adopting the necessary technology or it is not. Most would predict that those that are not will soon be left behind. This is one reason why we are seeing such consolidation of anesthesia practices; only those with access to significant capital resources can make the necessary investment in IT.
Maybe this is the wrong question. There is a paradigm shift taking place in medicine. We joke about the fact that physicians are not business people but the fact is this is not true: they tend to be true entrepreneurs focused on the success of their own little cottage industries. For far too long the consumer paid a premium for what economists refer to as supplier–induced demand. Only the doctor knew what was wrong with you and what it would take to make you better. This approach has resulted in the most expensive system on the planet with the least impressive results. Society wants consistent and predictable results for a reasonable cost. It wants a system that provides more accountability for outcomes in which specialists collaborate in the management of a patient’s care and to see evidence that all the impressive technology serves to make the system more effective and efficient, not just more expensive. It is a tall order, to be true, but it is what drives public policy which is where all these new regulations keep coming from.
Until providers start focusing on ways to make the entire system more cost-effective instead of on their share of the healthcare pie, they will find themselves swimming upstream in increasingly perilous waters. Fee for service medicine is destined to be replaced by a far more complicated system of risk-sharing. What we have seen thus far is just a preview of coming attractions. The public knows healthcare can be much better, and, frankly, most anesthesiologists believe that too. Those who find ways to make it so will be the real heroes of the next generation.
↧
How Well Does Measuring Anesthesiologists’ and other Physicians’ Quality Work?
particular, the ever-growing complexity of the Physician Quality Reporting Program (PQRS) and the newer Value Based Payment Modifier seems more likely to generate frustration than to lead to major improvements in healthcare safety and outcomes.
As noted in last week’s Announcement (The Anesthesia Conversion Factor and PQRS Changes in the Final Medicare Fee Schedule Rule for 2016), CMS is adding five items advocated by ASA to the list of PQRS measures that can be reported to a registry:
- Measure # 404: Anesthesiology Smoking Abstinence;
- Measure # 424: Perioperative Temperature Management (which revises and replaces Measure # 193);
- Measure # 426: Post-Anesthetic Transfer of Care Measure: Procedure Room to a Post Anesthesia Care Unit (PACU) (using a checklist or protocol);
- Measure # 427: Post-Anesthetic Transfer of Care: Use of Checklist or Protocol for Direct Transfer of Care from Procedure Room to Intensive Care Unit (ICU), and
- Measure # 430: Prevention of Post-Operative Nausea and Vomiting (PONV) – Combination Therapy.
Together with the current measures that will remain available for anesthesiologists’ PQRS reporting—Measure #76 (Prevention of Central Venous Catheter Related Bloodstream Infections) and Measure #44 (Preoperative Beta-Blocker in Patients with Isolated CABG Surgery; reportable only through a registry beginning in 2016)—and the various “cross-cutting” measures such as inquiring into the existence of an Advance Care Plan (Measure #47), at least one of which must be reported if the physician submits claims for any visit services, do the items on this list give real understanding into the quality of anesthesia care? And should they be the basis for financial incentives or penalties?
Ashish Jha, MD, MPH wrote on his blog An Ounce of Evidence on March 20, 2014 (What makes a good doctor, and can we measure it?) that the effective use of beta-blockers or good hemoglobin A1C control are important,
But I’m not sure they really measure the quality of the physician. They measure quality of the system in which the physician practices. You can have a mediocre physician, but on a good team with excellent clinical support staff, those things get done. Even the smartest physician who knows the evidence perfectly can’t deliver consistently reliable care if there isn’t a system built around him or her to do so.
The inability of current quality measures to capture the quality of the physician’s work is one of the factors considered by Sabriya Rice in her article Physician Quality Pay Not Paying Off published in Modern Healthcare on May 15, 2015. As various observers have noted, the science of measuring quality is still very immature—and thus linking the existing measures to compensation, Rice writes, “might be premature. Improvements seen on easily tracked process measures such as checklist use or giving discharge instructions may not lead to improvements in patient outcomes such as lower mortality and lower readmission rates.”
In addition to the lack of well-defined and actionable measures that make sense to the physicians being assessed, overly complex compensation designs and poor alignment of goals have led to disappointing results for a number of pay-for-performance programs. Not understanding the actual barriers to desired behaviors and results—lack of knowledge, resources or motivation, for example—is also an impediment. Rice cites several examples of programs that failed to deliver, including that of Fairview Health Services in Minnesota, which tied 40 percent of clinician compensation to performance on a suite of metrics required by state law, with salary increases based on overall group performance on benchmarks for diabetes, cardiovascular and asthma care and select cancer screenings. The compensation model was most effective with the poorest-performing physicians, who improved six times more than the higher performers. Overall, quality at Fairview improved no more than it did at competing system that did not institute any pay-for-performance programs.
On the other hand, some health systems are encountering success in paying their physicians for meeting quality measures and otherwise participating in population health improvement programs. Gregory A. Freeman, writing in the September 2015 issue of HealthLeaders magazine (Financial Incentives for Physicians), points to three such systems and to the lessons learned from each:
- Lodi Health, operating a single hospital in California, has been involved with Medicare’s Bundled Payments for Care Improvement Initiative for total joint procedures for two years. During the first year of participation, the only one for which results are currently available, Lodi’s costs covering 30 days of postoperative care came in under the CMS benchmarks in every quarter, enabling Lodi to share in the savings. Initially reluctant to collaborate in designing more standardized perioperative care, Lodi’s orthopedic surgeons are now showing interest in participating in the hospital’s gainsharing program and in the increased volume of cases going to the orthopedic surgeons who are already on board. What Lodi plans to do as it considers additional bundled payment initiatives is to secure earlier physician buy-in so that the doctors will help design and take ownership of the program.
- The chief medical officer at Texas Health Physicians Group, which counts nearly 850 primary care physicians in 250 clinics across the state, realized the importance of involving physicians from the beginning. The physicians wrote, and the organization adopted, a “compact” defining the parties’ expectations of each other and addressing topics such as clinical excellence. Among other things, the organization’s physicians are now required to demonstrate training and proficiency in high-reliability principles. The organization provides physicians with a data analysis tool that allows them to examine their own patient data and identify gaps in care and requires that they use the tool as a condition to participating in a new quality bonus program that offers up to 15 percent of salary for meeting 13 basic measures.
- At Bon Secours Health System in Marriottville, Maryland, all 250 physicians who were eligible for the Primary Care Quality Incentive Program launched this year opted to participate. The incentive is based on three components: citizenship (attending 75 percent of relevant meetings and completing required training on topics such as infection control and HIPAA); successful attestation to meaningful use of Bon Secours’ electronic health records, and compliance with the 33 quality measures for which Bon Secours is accountable as an ACO participating in the Medicare Shared Savings Program. If the physician only satisfies one or two of the three requirements, he or she is eligible for a partial bonus.
Unlike the pay-for-performance programs summarized above, Medicare’s PQRS has never had physician buy-in. The incentive payments have for many physicians been less than the costs of compliance. Now that there are no payments for meeting the requirements but only a penalty—which for some large practices may go as high as six percent based on performance in 2015—the calculus may change. Nevertheless, participation is apt to remain grudging as long as the measures do not equate to physicians’ own perception of quality. As stated in a Health Affairs Health Policy Brief on Physician Compare published online on December 11, 2014,
Physician accountability and quality improvement advocates complain that the field has been stuck for many years with too many measures of the processes of care and not actual patient outcomes. For example, it is important and relatively easy to measure how many patients in a group practice get a blood sugar test. More difficult but more meaningful is how many of that practice's diabetes patients suffer, over time, the problems (such as blindness and heart disease) that result from poor blood sugar control.
Indeed, after ten years of "measure development," most of the measures of physician performance still fall into the "process" category.
One vehicle that bypasses the issues of validity around individual physician quality measures is the Perioperative Surgical Home (PSH) model. “The overall goal of the PSH is to provide improved clinical outcomes and better perioperative service at lower cost.” (Kain ZN. et al., The Perioperative Surgical Home as a Future Perioperative Practice Model, Anesth Analg 2014;118:1126-1130.) The PSH route to improved clinical outcomes is the use of procedure-specific integrated care pathways and/or standardized clinical assessment and management plans (SCAMPs) rather than a set of process measures. (See Vetter TR, et al. The Perioperative Surgical Home: How Anesthesiology Can Collaboratively Achieve and Leverage the Triple Aim in Health Care, Anesth Analg 2014;118:1131-1136.) Measures have an important role to play in the PSH. Internally reported (private) measures—that is, measures of operational efficiency such as case postponement and cancellation rates, safety measures such as sepsis and patient experience measures such as prevention of postoperative nausea and vomiting—will provide the PSH members with performance information at the level of the organization, team or individual provider. Externally reported measures, including those available through the PQRS, “will demonstrate the success of the PSH concept over time, by showing an increase in the value of care.” (ASA Committee on Future Models of Anesthesia Practice, Perioperative Surgical Home Brief, 7/15/13). The real determinant of success in the various PSH initiatives developing around the country, however, will be the quantified improvement in patient outcomes and reduced costs through the PSH’s team-based system of coordinated care that guides the patient throughout the entire surgical experience. That improvement, and not the number of process measures checked off on a record created for traditional fee-for-service payment purposes, will be the best gauge of quality.
↧
Anesthesiologists Should Prepare for the Medicare Comprehensive Care for Joint Replacement (CJR) Payment Model
CMS has now finalized its proposal to cover total joint replacement (TJR) procedures through a bundled payment methodology. Under the Final Rule issued on November 16, 2015, some 800 hospitals across the country will be financially responsible for all of the inpatient and postoperative care of patients undergoing total knee or hip replacements from admission until 90 days after discharge. CMS estimates that the new bundled-payment test will cover about 23 percent of TJR surgeries for which Medicare pays and save Medicare $343 million over the five performance years of the model.
Through the Comprehensive Care for Joint Replacement (CJR) payment model, hospitals in 67 Metropolitan Statistical Areas (MSAs) will receive additional payments if quality and spending performance are strong or, if not, potentially have to repay Medicare for a portion of the spending for care surrounding a lower extremity joint replacement procedure. The goal of the CJR model, according to CMS’s press release, is “to give hospitals a financial incentive to work with physicians, home health agencies, skilled nursing facilities, and other providers to make sure beneficiaries get the coordinated care they need.” This creates an important opportunity for anesthesiologists to collaborate with their hospitals in improving outcomes for TJR patients and earning a CMS incentive payment. The CJR model may even, perhaps, be the impetus for launching a Perioperative Surgical Home.
The episode of care begins with an admission to a CJR hospital of a Medicare patient who is ultimately discharged under MS-DRG 469 (Major joint replacement or reattachment of lower extremity with major complications or comorbidities) or 470 (Major joint replacement or reattachment of lower extremity without major complications or comorbidities) and it ends 90 days post-discharge. The episode includes all related items and services paid under Medicare Part A and Part B for all Medicare fee-for-service beneficiaries, with the exception of certain exclusions.
Every year during the five performance years of this model, CJR hospitals will receive separate episode target prices for MS-DRGs 469 and 470. All patients in those two MS-DRGs will be included in the CJR program. CMS will also use a simple risk stratification methodology to set different target prices for patients with hip fractures within each MS-DRG.
All physicians and providers and suppliers involved in the care of the CJR patients will be paid under the usual rules and procedures of the Medicare program for episode services throughout the year. At the end of each model performance year, actual spending for the episode is compared to the Medicare target episode price for the particular hospital. Depending on the participant hospital’s quality and episode spending performance, the hospital may receive an additional payment from Medicare or be required to reimburse Medicare for a portion of the episode spending (after the first year, during which there will be no repayment imposed). CMS will limit how much a hospital can gain or lose based on its actual episode payments relative to target prices.
TJR surgeries are an obvious target for CMS as it moves toward its goal of having 30 percent of all Medicare fee-for-service payments made via alternative payment models by 2016 and 50 percent by 2018. As we noted in our August 24, 2015 Announcement discussing the proposed CJR rule, A Role for Anesthesiologists in CMS’s New Comprehensive Care for Joint Replacement Payment Program, Medicare spent more than $7 billion on more than 400,000 TJR procedures in 2013 and again in 2014. There is considerable variation in the costs of episodes of care, both between patients and on a geographic basis. The rate of complications, like infections or implant failures after surgery, can be more than three times higher at some facilities than others, increasing the chances that the patient may be readmitted to the hospital. And, the average Medicare expenditure for surgery, hospitalization and recovery varies from $16,500 to $33,000 across geographic areas.
The Final Rule, issued after CMS considered 400 comment letters filed in response to the Proposed Rule, contained a number of important changes. Among these are the following:
- Reduction in the number of MSAs in which the CJR program is mandatory from 75 to 67. (To determine whether a given hospital is in one of the 67 MSAs, go to Melanie Evans’s article How hospitals are prepping for Medicare's mandatory bundled-pay test at Modern Healthcare online, or download a spreadsheet listing all of the CJR hospitals.)
- Delay of the implementation date, to April 1, 2016. Numerous commenters asked CMS to delay the start of the model for a full year, to January 1, 2017, but CMS only granted a three-month reprieve.
- Application of composite quality scoring calculations, including consideration of patient-reported measures and hospital improvements in quality, that will be used to assign hospitals into acceptable, good and excellent quality categories for purposes of determining eligibility for gainsharing payments with CMS. In the Proposed Rule CMS had instead put forward a threshold methodology under which hospitals would need to meet or exceed the 30th percentile performance threshold in order to qualify for savings. Hospital performance will be evaluated on three measures:
- Total hip arthroplasty/total knee arthroplasty complications
- Hospital Consumer Assessment of Healthcare Provider Systems (HCAHPS) survey
- Patient-reported outcomes
- Risk stratification of the target price for each episode of care based on the patient’s hip fracture status.
The Final Rule does not address a topic of considerable concern to providers, the requested waiver of fraud and abuse rules that proscribe payments for referrals, i.e., the anti-kickback statute and the Stark law. It refers, however, to a special notice jointly issued by CMS and the OIG on November 16th describing the conditions under which waivers would be available for alignment payments under sharing agreements between participating CJR hospitals and “collaborators” such as physicians, distributions from physician practices to “practice collaboration agents” and patient incentives.
While hospitals and their national association did not welcome the CJR payment model, questioning CMS’s authority to make a bundled-payment program compulsory, there are several potential benefits for anesthesiologists and pain physicians.
First, physicians participating in CJR might be able to meet the requirements that would otherwise apply under the Merit-based Incentive Payment System (MIPS) that will replace current quality reporting programs in 2019 pursuant to the Medicare Access and Chip Reauthorization Act of 2015 (MACRA). Alternatively, they may qualify as “alternative payment model” participants as defined in MACRA and therefore be excluded from MIPS, through their participation in CJR. In the Final Rule, CMS suggested that it will address the question when it releases guidance on the implementation of MACRA next year.
Second, the CJR payment model presents an opportunity for anesthesiologists to step up and solve their participant hospital’s problem—the promise of a negative payment adjustment if the hospital does not meet the target for its TJR episodes—in return for a share of any bonus that they help the hospital earn. The CJR hospitals now have a clear incentive to listen to proposals on reducing the rate of complications and total spending through better coordination of perioperative care. Anesthesiologists should consider preparing and negotiating to lead their hospitals’ CJR work.
↧
↧
Stark 101 for Anesthesiologists
Sometimes those of us in the healthcare industry become so immersed in the multitude of applicable regulations, and their evolution and ambiguities, that we need to take a step back and be reminded of the basics. So for a few moments, let’s push aside the status of healthcare reform, the future of independent anesthesiology practices, the abstract and sometimes conflicting guidance governing anesthesia joint ventures and the nuances of ICD-10. Let’s refresh our recollection regarding a federal law that has been with us in various forms for about 25 years and that continues to impact us each day. This is a broad overview of the federal Stark law1 in 10 quick bullet points. 
- It’s important to understand what Stark is and what it is not. It is relatively common for healthcare attorneys to receive calls from clients requesting a Stark review of a relationship when the Stark law is not even at issue. For example, many services relationships between anesthesiologists and ambulatory surgical centers and the joint ventures between anesthesiologists and gastroenterology groups avoid implicating Stark but involve risk under applicable federal or state anti-kickback laws and state fee-splitting laws. These laws are not all the same. In order to analyze an arrangement and ensure legal compliance, it is crucial to understand which laws are truly applicable and which laws are not.
- The federal Stark law is a technical statute that requires a technical analysis. In order for a relationship to implicate Stark, five basic elements must be present: (1) a physician must make (2) a referral for the furnishing of (3) designated health services payable by Medicare (4) to an entity (5) with which he/she (or an immediate family member) has a financial relationship.2 When the Stark law is implicated, only the physician may make such a referral, and only the entity may present (or cause to be presented) claims for such referred services, if a Stark exception applies to protect the applicable financial relationship. Each arrangement must be analyzed on a case-by-case basis with close attention to the underlying circumstances.
- In the Stark context, intent (whether bad or good) doesn’t matter. Unlike the federal Anti-Kickback Law,3 which is a criminal law prohibition focused on impermissible intent, Stark is a strict liability civil statute. In other words, an honest good faith mistake can result in a Stark violation. And yes, this does mean that an inadvertent missing signature on a services agreement or an attorney’s failure to ensure that an agreement has a term of at least one year may alone prevent reliance on an available Stark exception and could, depending upon the circumstances, result in a relationship constituting a Stark violation that results in millions of dollars of overpayments.
- Understanding the applicable definitions is the key to any Stark analysis. Each element of the Stark law relies upon specific statutory and regulatory definitions that are clarified by regulatory preamble, case law and other federal guidance. For purposes of this brief article, we note that the term “physician” includes anesthesiologists (MDs and DOs); “designated health services” (or DHS) include without limitation certain inpatient and outpatient hospital services;4 and financial relationships may be direct or indirect and may include not only ownership and compensation relationships but also other relationships involving non-monetary remuneration exchanged between the parties.5
- Some (but not all) anesthesia arrangements implicate Stark. For example, in order for an arrangement to violate Stark, there must be a referral of DHS involved.6 It is common for anesthesiologists with pain medicine practices to order DHS in connection with their pain management services. Also note that the Centers for Medicare and Medicaid Services (CMS) has indicated that anesthesiologists (unlike other specialties such as hospital-based pathologists, radiologists, or radiation oncologists under certain circumstances) may be considered to have made referrals of DHS when they order the technical component of DHS performed by someone other than the physician.7 But also note that the Stark definitions of “inpatient hospital services” and “outpatient services” do not include “professional services performed by physicians, physician assistants, nurse practitioners, clinical nurse specialists, certified nurse midwives, certified registered nurse anesthetists and qualified psychologists, if Medicare reimburses the services independently and not as part of the inpatient or outpatient hospital service (even if they are billed by a hospital under an assignment or reassignment).”8
- Every element of a Stark exception must be satisfied in order for the exception to be helpful. There are numerous exceptions but reliance upon an exception requires that each and every element be satisfied. One common exception relied upon by anesthesiologists is, for example, the personal services arrangement exception.9 Broadly summarized, the personal services exception requires that (a) each arrangement is set out in writing, is signed by the parties, and specifies the services covered by the arrangement; (b) the arrangement covers all of the services to be furnished by the physician (or an immediate family member of the physician) to the entity; (c) the aggregate services contracted for do not exceed those that are reasonable and necessary for the legitimate business purposes of the arrangement; (d) the term of each arrangement is for at least one year; (e) the compensation to be paid over the term of each arrangement is set in advance, does not exceed fair market value, and, except in the case of certain physician incentive plans, is not determined in a manner that takes into account the volume or value of any referrals or other business generated between the parties; and (f) the services to be furnished under each arrangement do not involve the counseling or promotion of a business arrangement or other activity that violates any Federal or State law.
- In the Stark context, fair market value becomes not only a business term but also a legal term. As referenced above, demonstrating fair market value is often essential to ensuring that proposed arrangements are compliant with Stark.10 The definition of fair market value in the healthcare regulatory context is different than in other contexts. Although it is sometimes acceptable for the reasonable determination of fair market value and document such determination in their files, the best approach is to obtain a third party valuation from a qualified and experienced healthcare valuation consultant.
- Stark violations can have devastating consequences. As described above, when the Stark referral prohibition is violated (because Stark is implicated and there is no available exception), Medicare reimbursement is not available for the DHS services provided as a result of the prohibited referral. This can result in denials of payment or mandatory refunds of payment. Providers are required to report and return any resulting overpayment no later than 60 days after the date on which the overpayment was identified or the date on which any corresponding cost report is due, if applicable.11 Stark law violations can also serve as the basis for civil monetary penalties, False Claims Act liability (which may result in a qui tam suit and treble damages) and potentially exclusion from the governmental health care programs.12
- CMS has a protocol that providers may use to self-disclose a Stark violation. Note that CMS has adopted a Medicare self-referral disclosure protocol to enable providers to self-disclose actual or potential Stark violations. Despite the guidance and discretion available to CMS to mitigate the impact of a Stark violation, the self-disclosure process remains a very intimidating process for the health care community.13
- Stark calls upon anesthesiologists to act prudently. For anesthesiologists, it is crucial to seek legal guidance when there is any potential healthcare regulatory concern.14 Experienced health care attorneys will be able to assist in determining the actual legal issues and to advise whether a proposed relationship is defensible from a legal perspective. Relationships between anesthesiologists and hospitals or other facilities should always be documented in writing to reflect the entire relationship, be updated overtime as appropriate, be reviewed to confirm commercial reasonableness and be scrutinized to ensure that compensation is within the range of fair market value. When in doubt about whether the Stark prohibition is applicable to a proposed relationship, the parties should certainly err on the side of caution and satisfy each and every element of an available Stark exception or refrain from implementing the arrangement. Even when Stark is clearly not implicated, satisfaction of a Stark exception is typically advisable as a best practice and regulatory safeguard.
1 For purposes of this article, “Stark” refers to 42 U.S.C. §1395nn, and the regulations and guidance promulgated thereunder.
2 A discussion of Stark’s application to Medicaid claims is beyond the scope of this broad overview.
3 See 42 U.S.C. §1320a-7b(b) and the regulations and guidance promulgated thereunder.
4 “Designated health services” include clinical laboratory services, physical therapy services, occupational therapy services, outpatient speech-language pathology services, radiology and certain other imaging services, radiation therapy services and supplies, durable medical equipment and supplies, parenteral and enteral nutrients, equipment, and supplies, prosthetics, orthotics, and prosthetic devices and supplies, home health services, outpatient prescription drugs and inpatient and outpatient hospital services.
5 See 42 CFR §411.354. In the anesthesia context, financial relationships can involve, depending upon the circumstances, exclusive agreements with stipends or other compensation, ownership interests in ambulatory surgical centers and the receipt of other items of value such as space and equipment. See U.S. ex rel. Kosenske v. Carlisle HMA, Inc., 554 F.3d 88 (3d Cir. 2009).
6 For example, see discussion in Advisory Opinion No. 98-001 (1998) (regarding a proposed ambulatory surgical treatment center).
7 See Stark Phase III Final Rule preamble, 72 FR 51012, 51021 (2007).
8 See 42 CFR §411.351.
9 See 42 CFR §411.357
10 For example, for purposes of the Federal Stark law, “fair market value” means: “the value in arms’ length transactions, consistent with the general market value, and, with respect to rentals or leases, the value of rental property for general commercial purposes (not taking into account its intended use) and, in the case of a lease of space, not adjusted to reflect the additional value the prospective lessee or lessor would attribute to the proximity or convenience to the lessor where the lessor is a potential source of patient referrals to the lessee.” 42 U.S.C. §1395nn. The regulations promulgated pursuant to the Federal Stark law go on to state, “general market value” means: “…the price that an asset would bring as the result of bona fide bargaining between well-informed buyers and sellers who are not otherwise in a position to generate business for the other party, or the compensation that would be included in a service agreement as the result of bona fide bargaining between well-informed parties to the agreement who are not otherwise in a position to generate business for the other party, on the date of acquisition of the asset or at the time of the service agreement. Usually, the fair market price is the price at which bona fide sales have been consummated for assets of like type, quality, and quantity in a particular market at the time of acquisition, or the compensation that has been included in bona fide service agreements with comparable terms at the time of the agreement, where the price or compensation has not been determined in any manner that takes into account the volume or value of anticipated or actual referrals.” 42 C.F.R. §411.351 (emphasis added). For a discussion of fair market value principles as they relate to hospital exclusive contracts, see for example the Stark Phase II Interim Final Rule, 69 FR 16054 (2004).
11 ACA §6402.
12 See 42 U.S.C. §1395nn, 42 CFR §411.353 and 42 CFR §1003.100. See also for example In U.S. ex rel. Kosenske v. Carlisle HMA, Inc., 554 F.3d 88 (3d Cir. 2009) and the Covenant Medical Center 2009 False Claims Act Settlement (http://www.justice.gov/opa/pr/covenant-medical-center-pay-us-45-million-resolve-false-claims-act-allegations).
13 ACA §6409. See also https://www.cms.gov/medicare/fraud-and-abuse/physicianselfreferral/self_referral_disclosure_protocol.html.
14 An excellent resource for new or experienced physicians attempting to understand Stark and the federal fraud and abuse laws is “A Roadmap for New Physicians: Avoiding Medicare and Medicaid Fraud and Abuse,” which is available at http://oig.hhs.gov/compliance/physician-education/index.asp.
↧
Update for Anesthesiologists on the Value Based Payment Modifier
CMS released the Final Medicare Fee Schedule Rule for 2016 on October 30, 2015. The November 9th issue of F1RSTNews discussed the conversion factors for anesthesia ($22.4426) and for other services ($35.8279) and some of the changes to the measures and registry options for the Physician Quality Reporting System (PQRS). The final rule addresses a number of other matters of interest to anesthesiologists and pain physicians. In this issue, we will summarize developments concerning the Value Based Payment Modifier (VM).
The VM adjusts Medicare fee-for-service payments either upward or downward by assessing both the quality of care and the cost of the care provided, as explained in our November 3, 2014 Alert What Anesthesiologists Need to Know about the Value-Based Payment Modifier. It is an adjustment made on a per claim basis to Medicare payments for physician services. It is applied at the Taxpayer Identification Number (TIN) level to physicians (and beginning in 2018, to non-physician Eligible Professionals [EPs]) billing under the TIN.
Required under the Affordable Care Act, the VM began to be phased in in 2015 (based on 2013 performance). It will be fully implemented in 2017 and will continue in effect through 2018—and then will be phased out again and replaced by the Merit-Based Incentive Payment System (MIPS) in 2019.
The VM program aligns with the PQRS and includes a payment adjustment based on PQRS reporting: EPs who do not satisfactorily report enough PQRS measures to avoid the PQRS penalty will receive an additional penalty under the VM program. For EPs who avoid the PQRS penalty, CMS determines the VM through a quality-tiering process using PQRS participation information, CMS-calculated outcomes related to hospital readmissions and hospital admissions for certain chronic and acute conditions, and also certain cost measures to assign two composite scores to each medical group: a quality composite and a cost composite. Each score will be classified as “high,” “average” or “low” based on a comparison to national averages. This quality tiering will determine if group performance is statistically better, the same as, or worse than the national mean, based on standard deviation calculations. In payment year 2018, the maximum bonus for high-quality/low-cost performers will be 4.0x, x being the upward adjustment payment factor. The upward adjustment payment factor will be determined in budget neutral fashion by the aggregate amount of penalties imposed on low-quality/high cost practices. The maximum penalty for high-cost/low quality providers will be -4 percent.
The gradual implementation of the VM has been based on the number of EPs in the practice. Only groups with 100 or more EPs are receiving payment adjustments this year. In 2016, the VM will affect payment to groups with 10 or more EPs, based on their performance in 2014. CMS will begin to apply the VM to payments to all physicians, including those in solo practice, in 2017 reflecting their performance in 2015. The Final Rule expands on the types of EPs included in the program by finalizing a proposal to apply the VM to certified registered nurse anesthetists (CRNAs), nurse practitioners, physician assistants and clinical nurse specialists. The table below shows the evolution of the maximum adjustments allowed per year, the group sizes and the EPs to which they apply:
Maximum Payment Adjustments Per Year, Per Group Size and Per Type of EP

Thus,
- All group practices and solo practitioners will be subject to upward, neutral or downward adjustments derived under the Value Modifier quality-tiering methodology, except group practices comprised solely of nonphysician providers (NPPs). NPPs who are solo practitioners will be held harmless from downward adjustments.
- The maximum upward adjustment under the quality-tiering methodology shall be +4.0 times an adjustment factor (to be determined after the conclusion of the performance period) for groups with ten or more professionals, and +2.0 times an adjustment factor for all other groups and solo practitioners.
- The maximum downward adjustment for 2018 shall be -4.0 percent for groups with ten or more professionals and -2.0 percent for all other groups and solo practitioners (with the exception of NPP-only groups and NPPs who are solo practitioners).
- For all groups and all EPs, being classified as “average quality/average cost” will produce a 0.0 percent VM adjustment. For further detail of the potential adjustments by group size and type of EP, MGMA members may consult the MGMA’s Exclusive Analysis of the 2016 Medicare Physician Fee Schedule. MGMA’s The Value-Based Payment Modifier: How to Prepare Your Practice, written in December 2014, is an excellent introduction to the VM program.
Most anesthesiologists and CRNAs are unlikely to be tiered as anything but average on either quality or cost. The PQRS measures that they report are just part of the composite quality score. The other components are:
- Composite of rates of potentially preventable hospital admissions for three chronic conditions: heart failure, chronic obstructive pulmonary disease and diabetes;
- Composite of rates of potentially preventable potentially preventable hospital admissions for three acute conditions: dehydration, urinary tract infections and bacterial pneumonia, and
- All-cause readmissions within 30 days of discharge from an acute care hospital.
For any of these outcome measures to apply, the clinician or the clinician’s group must have furnished a plurality of the beneficiaries’ primary care services and there must be a minimum of 20 attributable cases. Similarly, for two of the three cost measures, CMS will use a minimum case size of 20 and the attribution process that assigns a beneficiary to the TIN providing more primary care services to that beneficiary than any other TIN. These two cost measures are:
- Total Part A and Part B per capita costs for all Medicare patients, and
- Total Part A and Part B per capita costs for patients with specific conditions (heart failure, coronary artery disease, chronic obstructive pulmonary disease and diabetes).
The third cost measure is CMS’s evaluation of the “Medicare Spending Per Beneficiary” (MSPB), which covers the Part A and Part B costs spanning three days prior to and 30 days after an inpatient hospitalization. Beneficiaries are attributed to the group that provided the plurality of Part B services during the inpatient stay—but the TIN must have 125 or more MSPB episodes for the measure to be included in the cost composite, and again, few if any anesthesia groups will meet this requirement.
There is not much, therefore, that anesthesiologists or CRNAs can do to affect their quality-tiering under the VM next year. They can and should try to ensure that they report satisfactorily under the PQRS program to avoid the penalties: -4 percent under the VM plus -2 percent adjustment under the PQRS itself, or a total of -6 percent for groups of 10 or more EPs, and -2 percent (VM) plus -2 percent (PQRS), or a total of -4 percent, for smaller groups including at least one physician. All EPs who do not successfully participate in the PQRS in 2016 will receive a -2 percent adjustment.
The VM and PQRS programs have both become hopelessly complex, in our opinion. Individual physicians’ and groups’ Feedback Reports and Quality and Resource Utilization Reports (QRURs), which should help physicians to understand and improve their performance, are full of inconsistencies and errors; this has led CMS to extend the deadline for filing informal appeals several times, the latest being December 16, 2015. Extending the deadline to appeal is not enough, as many physicians are not aware that they are facing significant Medicare payment reductions that they could, and should, contest. In a letter dated December 1, 2015, the American Medical Association pointed out the communications and analyses flaws in CMS’s calculations of penalties to be applied to 2016 payments, and it called upon CMS Acting Administrator, Andrew M. Slavitt to apply a broad “hold harmless” policy that would automatically exempt all physicians who attempted to comply with the 2014 PQRS requirements from any PQRS or VM penalties in 2016. Such is, unfortunately, the state of the PQRS and VM programs.
↧
What Does “Patient Satisfaction” Mean to and for Anesthesiologists?
“Patient satisfaction” and the patient experience are considered key measures of quality and performance in our increasingly value-based healthcare system. The American Society of Anesthesiologists’ Committee on Performance and Outcomes Measurement (ASACPOM) has acknowledged that “monitoring of patient satisfaction has already been incorporated into payment for performance plans and will be an important component of other payer, healthcare plan affiliations. It is a given that this trend will continue and that assessment of patient satisfaction will affect payment for anesthesiologists in the near future.” (White Paper on Patient Satisfaction and Experience with Anesthesia, as revised June 9, 2014.) Health plans use patient satisfaction surveys to evaluate physicians and to determine incentive compensation, and consumer web sites such as HealthGrades often report patient satisfaction ratings as the sole physician measure. Patient satisfaction surveys are also playing a growing role in medical boards’ assessment of physicians’ competency.
The ASA-Anesthesia Quality Institute’s Qualified Clinical Data Registry (QCDR) provides for reporting of a “Composite Anesthesia Patient Experience Measure” with the following description: Percentage of patients, aged 18 and older, who were surveyed on their patient experience and satisfaction with anesthesia care (e.g. private vendor assessment of patient experience and satisfaction, Consumer Assessment of Healthcare Providers and Systems Surgical Care Survey or S-CAHPS).”
Successful participation in Medicare’s Physician Quality Reporting System (PQRS) next year will require practices of 100 or more eligible professionals (EPs)s that are participating in the Group Practice Reporting Option (GPRO) to report the CAHPS for PQRS survey data. Practices of 25-99 EPs that registered in the GPRO have the option of supplementing PQRS reporting with the CAHPS for PQRS survey. The CAHPS for PQRS survey will count for three of the requisite nine measures and one National Quality Strategy domain.
Starting in 2016, CMS plans to begin voluntary monthly data collection using the new Outpatient and Ambulatory Surgery Consumer Assessment of Healthcare Providers and Systems (OAS CAHPS) survey tool. The official OAS CAHPS survey, certified by the Agency for Healthcare Research and Quality, includes 37 questions that assess patient experience measures for hospital-based outpatient surgery departments or free-standing ambulatory surgery centers. The survey, to be administered by Press Ganey, will include questions about the check-in process, the facility environment, the patient's experience communicating with administrative staff and clinicians, attention to comfort, pain control, how well pre- and post-surgery care information is provided, the patient's overall experience and patient characteristics.
For all that the measurement of patient satisfaction is a now fact of our professional lives, its value is not fully accepted. Many anesthesiologists “question whether assessment of patient satisfaction with anesthesia services is meaningful or can improve quality,” as the ASACPOM stated in the Introduction to its White Paper.
In The Cost of Satisfaction: A National Study of Patient Satisfaction, Health Care Utilization, Expenditures, and Mortality (J. Fenton et al., Arch Intern Med. 2012;172(5): 405-411), a study involving a nationally representative sample, the authors found that higher patient satisfaction was associated with greater inpatient use, higher overall health care and prescription drug expenditures, and increased mortality, albeit with less emergency department use. The most satisfied patients also had statistically significantly greater mortality risk compared with the least satisfied patients. The disadvantages of using patient satisfaction as a proxy for quality include the facts that physicians whose compensation is more closely linked with patient satisfaction are more likely to deliver discretionary services, such as advanced imaging for acute low back pain, and that discretionary services may lead to iatrogenic harm via overtreatment, labeling or other causal pathways. At a minimum, reviewing the data leads to the conclusion “that we do not fully understand what drives patient satisfaction as now measured or how these factors affect health care use and outcomes.”
The authors of a recent article published in the Hastings Report ("Patient-Satisfaction Surveys on a Scale of 0 to 10: Improving Health Care, or Leading It Astray?," Hastings Center Report 45, no. 3 (2015): 43-51), argue that the surveys could eventually compromise the quality of care and raise health care costs. "The pursuit of high patient-satisfaction scores may actually lead health professionals and institutions to practice bad medicine by honoring patient requests for unnecessary and even harmful treatments," they write. "Patient satisfaction is important, especially when it is a response to being treated with dignity and respect, and patient-satisfaction surveys have a valuable place in evaluating healthcare. Nonetheless, some uses and consequences of these surveys may actively mislead health care."
On the other hand, as the ASA CPOM observes in the White Paper cited above, measuring patient satisfaction may be associated with fewer adverse consequences in anesthesiology:
While higher patient satisfaction has generally been associated with increased testing, hospitalizations and invasive procedures, assessments of specific inpatient experiences may prove to be a notable exception. Using the Hospital Compare database, a recent study found an inverse relationship between patient experience and complication rates when assessing specific inpatient admissions, suggesting that lower complications are associated with improved experience and potentially vice versa. Thus, patient satisfaction scores may hold increased relevance for perioperative practitioners.
Perhaps the best strategy for anesthesiologists, given the ubiquity of patient satisfaction reporting requirements—as well as the QCDR percentage-of-patients-surveyed measure—is simply to be able to recognize good methodologies and to seek to steer one’s practice, institution and even payers to the best available instruments. Barnett et al. (Patient Satisfaction Measures in Anesthesia: Qualitative Systematic Review. Anesthesiology 2013; 119:452–78) undertook a systematic review of a very large number of studies and found a large number of well-developed tools to measure satisfaction with perioperative anesthesia care, but commented that “Perhaps our most significant finding is that the vast majority of anesthesia-related studies do not use validated tools to measure satisfaction, where this outcome is thought to be of importance.” The authors were unable to recommend any single survey or tool.
The ASA CPOM, however, has developed recommendations for a set of survey questions for use by anesthesia practices to report to the Anesthesia Quality Institute; the Committee “will also use these recommendations to engage both CMS and the AHRQ [Agency for Healthcare Research and Quality] in the revision of existing survey or development of new surveys that report on patient experience with anesthesia.” The recommendations cover four collection categories:
General information about the survey and the surgical procedure, e.g., survey type and method of administration, time between procedure and survey response, primary anesthesia type;
Patient demographic information, used for case-mix adjustment;
“Questions for a short form version of an anesthesia satisfaction survey intended to be added to another survey of patient satisfaction that does not assess satisfaction with anesthesia services,” and
Questions for a long form, stand-alone anesthesia satisfaction survey instrument.
The Appendices to the White Paper contain sets of questions in each of these categories. The White Paper is an important summary of and contribution to the literature on anesthesia patient satisfaction surveys. It should be very helpful to any anesthesia practitioner or researcher who wishes to understand the current tools available for assessing patient satisfaction or the open questions that will be resolved in the near future.
↧