The late great Yogi Berra was famous for his humorous and wise observations. It is true that “the future ain’t what it used to be.” Until a few years ago, the future did not encompass the perioperative surgical home (PSH), but the potential impact of the PSH model cannot be doubted now. It is hard, if not impossible, to argue with the relevance of the model as value-based purchasing takes hold within the governmental and private payer markets.
The lead article in this issue, The Perioperative Surgical Home: “Right for our Group?” by Rick Bushnell, MD, MBA, a private practice anesthesiologist in Southern California, is a shining example of the response that the proponents of the PSH hoped to bring about. The PSH is emphatically “right” for Dr. Bushnell’s group—a single specialty private practice, which, like many others, has been successful at providing traditional surgical anesthesia care but is wondering not just how to survive, but rather whether “this is the best we can do.” This is such a refreshing perspective: the PSH seen as an opportunity “to elevate our own practice of anesthesia” and as something much more than a defensive strategy. Because the three-minute pre-op interview often shortchanges the patient and the patient-anesthesiologist relationship, Dr. Bushnell’s group plans to place a physician in the clinic to see patients both pre-operatively and following discharge. The group has recognized that anesthesiologists must expand their skill sets in order to be effective in providing pre-op and post-op care. By the time you read this, Dr. Bushnell’s group will have participated in a PSH strategy meeting hosted by one of their hospitals. We look forward to keeping you posted on the progress of the venture in a series of follow-up articles.
The future not being what it used to be, but being, in fact, much more challenging, anesthesia practices must have leadership that is performing well. Readers who serve on their groups’ Boards of Directors will probably recognize some of the behaviors that can undermine performance in the newest article by Will Latham, MBA, CPA, of Latham Consulting Group: Improving Board Performance. They will also benefit from seeing to it that present and potential Board members understand their role and responsibilities, which Mr. Latham lays out succinctly while also explaining when and how to remove dysfunctional Board members.
Many anesthesia group Boards will at one time or another contemplate a practice-related financial relationship that implicates the federal Stark law. Over the last 25 years, an impressive mythology has grown up over what is, and what is not, a Stark violation. Understanding the basic principles of this complicated law is important, if only to avoid wasting time worrying about how it might apply when it actually is not in issue, and the 10-point primer offered here by Kathryn Hickner, JD of Ulmer & Berne, LLP (Stark 101 for Anesthesiologists) will help groups focus on what they need to know.
A less familiar legal risk for anesthesia groups that offer retirement programs including 401(k) plans is the responsibility of the plan fiduciary. The fiduciary may be a member of the group, or the group may engage an investment firm or professional. Patrick Runyen, CPA, CFP of Independence Advisors sets out some of the liabilities to which anesthesia groups, as plan sponsors, may be exposed in Managing the “L” Word in Your Practice’s Retirement Plan (Liability, That Is).
The future is not what it used to be in the realm of anesthesia practice management, either, ABC Vice President Jody Locke reminds us in Anesthesia Informatics: The Future is Upon Us. Whether we like it or not, “while a pen, an anesthesia record and a good billing agent used to be the essential keys to financial success, a whole new set of high-tech tools is becoming necessary”— specifically with the requirements of PQRS and QCDR reporting, the meaningful use program and ICD-10 coding. Those new tools will also be called for participating in alternative payment models forthcoming from Medicare. Although few anesthesiologists are participating in the early versions of these models, which ABC Vice President Joette Derricks summarizes in A Basic Primer on the Bundled Payments for Care Improvement Initiative, reviewing the fundamentals of the BPCI Initiative will held to prepare readers for the further efforts CMS is going to undertake to meet its goal of having 50 percent of Medicare payments in alternative payment models by 2018.
One cannot help but ask the question raised by Mr. Locke: “At what point does the provision of care become less relevant than the documentation of the care?” The question is, of course, rhetorical at this point. Anesthesia practices simply must make the necessary investments in information technology and accept their responsibility for seeking to make healthcare accountable and more cost-effective. Jessica KoImage may be NSFW. Clik here to view.vash, CHTSPW, of Koratek Perioperative Consulting, LLC takes a pragmatic look at anesthesia information management systems in her article Ensuring the Hospital’s AIMS Produces the Business Information Your Practice Needs. Whether your hospital is looking at a new AIMS implementation or already has an AIMS in place, there are steps you can take to make sure it turns the data captured by the system into the business information your practice needs.
Changing healthcare delivery models and payment systems, and the information technologies that are ever more integral to the new models, present us with enormous opportunities as well as challenges. We take comfort in the conclusion that most anesthesiologists, like the public, know that healthcare can be much better. I, for one, believe that we are getting there.
As we barrel toward the end of 2015, let us stop briefly to consider some predictions for the year ahead in healthcare. Below is a set of ten predictions that appeared in Fortune magazine earlier this month, along with several comments.
The Federal Trade Commission (FTC) will block a major hospital merger based upon data showing clearly that consolidation leads to price increases more than quality gains.
In fact on December 18th the FTC moved to block a proposed mega-merger between Advocate Health Care and NorthShore University HealthSystem in Illinois—the third hospital deal the FTC sought to block in the past seven weeks. The Illinois Attorney General joined the FTC in filing for a preliminary injunction to halt the merger pending Commission review. The Illinois systems, which, if the merger went through would have a combined 15 acute-care hospital campuses, a children's hospital and a large group of employed and affiliated doctors in the Chicago area, immediately said they would fight back. A final decision by the FTC Commissioners is expected to take at least a year; the loser will probably appeal through the federal courts. (Schenker L. FTC challenges NorthShore, Advocate Mega-Merger in Illinois. Modern Healthcare, December 18, 2015.)
On the other hand, as Philip Betbeze argues inHealthcare Delivery in 2016: A Lot of 'Little Somethings' Are Going to Happen(HealthLeaders Media, December 18, 2015), “infinitely more interesting [than the health system mega-merger] are the numerous combinations struck as providers seek to gain the greater scale and scope necessary to compete for contracts from those insurers and others, as well as being positioned to deliver better on an increasingly value-focused CMS, which has promised to tie 90 percent of all traditional Medicare payments to value by 2018. These hundreds of smaller deals are illustrative of an industry that's being remade beneath the surface as 2016 is upon us.” There could be many arrangements between health systems to work together on specific strategic initiatives such as “ACO creation, building a continuum of care in the region, incorporating new value-based plans directly with employers, sharing of other resources, leveraging different sites of care to equalize patient volumes among facilities, and, of course, starting a health insurance plan, just to name a few.” Anesthesiologists should hope and expect to play important roles in the launch of such initiatives.
A new type of wearables will include substitutes for more expensive medical therapies, i.e., “'Wearables’ become ‘Ther-ables.’” They will offer less invasive but highly effective treatments for diseases. They will also reflect a business model based upon the creation of medical value, as opposed to wellness, entertainment and education.
End-of-life care will be in the news and hospice use will double among accountable care organizations (ACOs) and capitated physicians. High deductible health plans and new payment models—not to mention increasingly expensive treatments—will make it necessary for physicians to engage in more end-of-life discussions with patients. One consequence, according to Fortune, will be increased pressure on drug pricing. Another will be higher incomes for physicians.
Anesthesiologists may undertake more responsibilities in the related areas of hospice and palliative care particularly as the Perioperative Surgical Home (PSH) model takes root. In her article Palliative Care and the Perioperative Surgical Home (ASA Monitor 11 2015, Vol.79, 28-30) , Kristin Fortner, MD notes that “In 2006, the American Board of Anesthesiology acknowledged certification in Hospice and Palliative Medicine, formally designating it a medical specialty open to anesthesiologists. As of 2014, there were 78 ACGME-accredited fellowships and 111 certified anesthesiologists. But the number of fellowship-trained and board-certified anesthesiologists practicing palliative care is a much smaller number, probably on the order of 20.” Fortner argues that “the need and opportunities for palliative-trained anesthesiologists, especially, have never been higher.”
A major hospital system will divest itself of its employed doctors, having avoided the move into risk-based reimbursement and losing too much of its investment. In the wake of such a divestiture, hospitals will begin unwinding the money-losing practices they have been acquiring over the last five years, much like the 1990s when physician practice management roll-ups failed.
The insurance innovation mania of 2015 will die down in 2016. Several provider-sponsored health plans and startups will find it hard to offer competitive premiums and, as a result, will attract few members and will hemorrhage cash. The “laws of physics” of health insurance favor large health plans that can use their market power to exact greater provider discounts and can use case managers to control their high-cost patients.
The excitement over “precision medicine” will abate because “biology is too complex, and care is simply not reliable enough to benefit from the fine-tuning imagined by precision medicine.”
Hospitals will cut back on their use of population health analytics and some analytics companies will disappear because their current customers cannot obtain enough value from their analytics tools. “In fact, most of the current value from these tools comes from upcoding and gaming the risk—adjustment system for higher payment as opposed to complication avoidance. In addition, most providers already know which of their patients are high risk, making these tools dispensable.”
The high cost of on-demand healthcare will reduce the attractiveness of this option. High customer acquisition cost combined with the limited ability of most people to pay high prices will shrink the market for on-demand doctors and prescription drug delivery. The high retail prices of traditional and on-demand care will help telemedicine to gain popularity, however, as patients actively seek increased access to care at lower cost.
ACOs are expected to increase the use of telemedicine as a way to achieve greater cost savings while improving patient care quality. (Lacktman N. 2016 Will be the Year of Telemedicine and ACOs. Health Data Management, December 21, 2015.) Telemedicine will also offer more and more applications for the preoperative and postoperative phases of the PSH model.
PCSK9 cholesterol drugs will make Sovaldi look cheap. PCSK9s are uniquely able to lower cholesterol to minuscule levels. The success of weekly injections will improve patient compliance, leading to more innovation in drug delivery strategies that limit the risk of patients forgetting to swallow pills.
Employers will start imposing rules to hold down spending on employee health. Fortune foresees that “Large employers may choose which doctors and hospitals employees visit, require second opinions before high cost procedures or treatments, recommend telemedicine before going to an emergency room, or require online tools for managing their conditions and out-of-pocket expenses.”
To the above list of Fortune’s predictions we would add a few of our own: more state legislative initiatives aimed at protecting patients who go out of network from balance or “surprise” billing; more data breaches like the one announced by Anthem in February 2015, in which hackers accessed the personal data of more than 80 million patients); ever-increasing consumerism and transparency of both prices and quality metrics, and more involvement of ambulatory surgery centers in PSH affiliations. Solid leadership in anesthesiology departments and groups will be more necessary than ever—and so will the potential rewards.
We begin this new year with a list of the key changes to CPT coding and Medicare payment policies.
The 2016 CPT edition had more than 300 changes, including 140 new codes, 132 revised codes and 91 deleted codes. It is important to understand the changes and what should be documented to support the new or revised codes.
The majority of changes for 2016 appear in the Pathology/Laboratory section of CPT. Radiology also had major CPT changes, including several for bundling along with “written report” guidelines. There have been gastrointestinal changes made in both 2014 (upper) and 2015 (lower) and in 2016 there were several additional changes. The Office of the Inspector General (OIG) has included non-covered services under Anesthesia Services to the 2016 Work Plan, stating: “We will review Medicare Part B claims for anesthesia services to determine whether they were supported in accordance with Medicare requirements. Specifically, we will review anesthesia services to determine whether the beneficiary had a related Medicare service. Medicare will not pay for items or services that are not ‘reasonable and necessary.’”
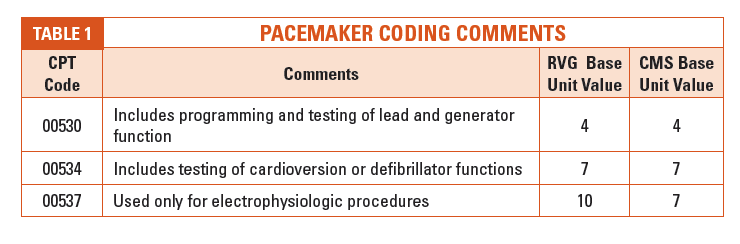
Medicare will continue to cover 100 percent of the allowable amount for screening colonoscopies as it has done since January 1, 2015. Patients will still be responsible for co-payments and deductibles for diagnostic and therapeutic colonoscopies, as well as co-payments for screening colonoscopies that end up with a biopsy or polyp removal. CMS finalized modified regulations relating to the 2015 policy change, confirming that the beneficiary deductible will be waived for anesthesia services furnished in conjunction with a colorectal cancer screening test even when a polyp or other tissue is removed during a colonoscopy. Specific modifiers must be reported in conjunction with the anesthesia code 00810. The modifiers are 33, screening colonoscopy and PT, screening colonoscopy converted to a therapeutic colonoscopy. Documentation should be clear on the reason for the procedure and the outcome of the procedure to code the modifiers appropriately. The following chart shows the use of the modifiers for code 00810, anesthesia for lower intestinal endoscopic procedures.
Again, there were no changes made to the anesthesia CPT codes, but there were additions and revisions to the ASA 2016 CROSSWALK. Anesthesia providers should ensure that they understand the impact of potential revenue or compensation changes due to additions or revisions to the ASA 2016 CROSSWALK (Please refer to Appendix A - Summary of Additions and Revisions in the 2016 ASA CROSSWALK for a complete list of the additions or revisions). These changes include CPT to ASA cross changes and alternative ASA code changes, and due to these changes the base unit values have been increased or decreased based on the change itself. For example, anesthesia for certain catheter placement services (36221-36226) was valued at 6-10 base units, depending on which of three different ASA codes (01924-01926) applied, and they have all been changed to cross to one ASA code, 01916, for 5 base units.
Pain management providers should take note of a few changes in the 2016 CPT code set. These include new paravertebral block/catheter codes along with additional bundling of imaging guidance with base CPT codes. Additional parenthetical guidelines have been added for destruction codes (64633-64636) due to common misconceptions. P - Revised indicates that only the parenthetical guidelines were revised, + denotes an add-on code.
In 2015 two new Evaluation and Management (E/M) codes were introduced that may have an impact on some anesthesiologists and the services they provide. CMS did not reimburse for these codes in the calendar year 2015; effective January 1, 2016, however, they have been assigned an active rate of reimbursement.
In 2015, Medicare made significant and substantial adjustments in the relative values that resulted in reimbursement changes. One of particular interest to pain medicine was the revision to the epidural steroid injections (62310, 62311, 62318, & 62319). In 2014 the reimbursement was drastically reduced and in 2015 Medicare realized that the services were potentially misvalued in 2014, therefore the RVUs for these services were adjusted in 2015 to include the fluoroscopic guidance. Due to this decision, Medicare prohibited separate billing of image guidance in conjunction with these services. An interesting point was the CPT 2015 Codebook does permit the separate reporting of fluoroscopic guidance, if used, with codes 62310, 62311, 62318, and 62319. However, the second quarter of 2015 NCCI edits included the bundling of these combinations for those carriers that have adopted NCCI edits. Even more interesting is that CPT 2016 Codebook still permits the separate reporting of fluoroscopic guidance with the four steroid injections. Rumor has it this may change in the near future with an errata notification.
A Few Reminders Regarding Your Clinical Documentation
Moderate (Conscious) Sedation is billed based on the intra-service time which starts with the administration of the sedation agent(s), requires continuous face-to-face attendance, and ends at the conclusion of personal contact by the physician providing the sedation. Since moderate sedation is a time-based code the intra-service time must be documented in the medical record. In order to bill for the first 30 minutes of intra-service time using code 99144, at least 16 minutes must be documented. An additional level, 99145, can be billed if 38 minutes of time are documented (each additional 15 minutes needs a minimum of 8 minutes).
Radiology was a subject of change for 2016 with several code changes. The biggest change for anesthesia and pain management is the use of imaging guidance. The following statement has been added to the Introduction, Surgery and Medicine sections in the CPT 2016 Codebook: “When imaging guidance or imaging supervision and interpretation is included in a procedure, guidelines for image documentation and report, included in the guidelines for radiology (including nuclear medicine and diagnostic ultrasound) will apply.” The radiology section also includes a new statement for “written reports,” i.e., “A written report (e.g., handwritten or electronic) signed by the interpreting individual should be considered an integral part of a radiologic procedure or interpretation. “Images” refer to those acquired in either an analog (i.e., film) or digital (i.e., electronic) manner.” The image interpretation and report should include the details of what the imaging was used for, the outcome of the use of the imaging, along with the medical necessity and documentation that the image is on file/stored/saved, etc. (the word “image” has replaced “film” in the radiology section.)
It is important to include documentation of the patient’s physical status and any co-morbidities on all anesthesia records. Often this information helps to support the medical necessity of the need for anesthesia and in some cases it may result in additional revenue.
ICD10 finally went into effect on October 1, 2015. ABC prepared for this implementation well in advance which has turned out to be a wise decision as the transition has been smooth. Remember to be as specific as possible in the diagnosis description when documenting and to include the condition, site/laterality, cause (how the injury/health condition happened, placed, activity, etc.), and qualifier (reason for or due to along with special details such as with/without bleeding/hemorrhage/obstruction, etc.) as applicable for each service performed. ABC clients may use our ICD10 hotline telephone number (1-800-544-6647 #1) as well as an e-mail address (ICD10.HelpDesk@Anesthesiallc.com) to assist with any ICD10 related questions.
We hope that all of our readers will have a happy, healthy and successful New Year.
More than 14 million screening colonoscopies are performed each year. Anesthesiologists and nurse anesthetists participate in a large proportion of these procedures. There are several developments that may bring down the numbers or at least slow the rate of growth of screening colonoscopies that our readers, especially those whose practices include a significant volume of anesthesia for colonoscopy services, should note.
The first of the changes going forward is the reduction of Medicare payments for lower gastrointestinal endoscopies that went into effect on January 1, 2016. CMS announced, in the Final Fee Schedule Rule issued in November 2015, that it was reducing the relative value units (RVUs) for the physician-work component of the Fee Schedule payment for screening colonoscopies by nine percent, from 3.69 to 3.36 RVUs, the value recommended by the AMA/Specialty Society Relative Value Update Committee (RUC). There were also changes to the RVUs for practice expenses. The resulting payment amounts and the decrease from 2015 to 2016 are shown below:
The majority of endoscopic procedures are performed in “Facilities” (ASCs, certified endoscopy clinics and hospital outpatient departments) and not in private physicians’ offices, so the cut for most gastroenterologists will be on the order of 9.5 percent for screening colonoscopies alone. The RVUs and hence the payment amounts for other lower GI endoscopies were reduced by as much as 17 percent. The predictable response from the gastroenterologists’ associations, as reported in the CMS explanation of its decision, was:
Many commenters expressed concerns that the proposed values for the lower GI code set will hinder efforts to reduce the incidence of colorectal cancer through detection and treatment by limiting access to screenings. Comments stated, “According to a poll of more than 550 gastroenterologists, more than half of the respondents plan to limit new Medicare patients if the proposed cuts are implemented; 55 percent plan to limit procedures to Medicare patients; and 15 percent are considering opting out of Medicare entirely. These findings suggest that GI physicians may not be able to maintain the current mix of Medicare patients and protect the financial viability of their practices.”
Further reductions in payment will be introduced as early as 2017 if CMS follows through on its plans to remove the value of moderate sedation from the codes that currently include it, including most of the GI endoscopy codes.
If the endoscopists reduce the number of screening colonoscopies that they perform on Medicare patients, there will be a concomitant decrease in the demand for anesthesia for these services. There are anesthesia practices whose case mix consists predominantly of anesthesia for lower GI endoscopies and whose business plans might potentially be affected.
Moreover, CMS has foreshadowed reductions in payments for anesthesia for colonoscopies. In the Final Rule, CMS noted that a separate anesthesia service is now billed to Medicare in more than 50 percent of colonoscopies and announced that “Given the significant change in the relative frequency with which anesthesia codes are reported with colonoscopy services, we believe the relative values of the anesthesia services should be re-examined.” The Agency plans to continue reviewing information, e.g., from the RUC, on whether anesthesia for upper and lower GI endoscopies is in fact “potentially misvalued.”
The ASA has vehemently protested CMS’s assumption that higher utilization levels means that CPT codes 00740 (anesthesia for upper GI endoscopy) and 00810 (lower GI endoscopy) are misvalued. The change that took effect on January 1, 2015, waiving Medicare patients’ co-payments and deductibles for some screening colonoscopies is evidence that CMS understands the public health imperative of increasing the number of patients who seek screening. (See ASA letter to CMS with “comments” on the proposal that was adopted in the Final Rule.) Nonetheless, CMS is highly likely to proceed with determining new RVUs for the procedures, which might be in place as early as next year.
Only one in three patients between the ages of 50 to 75 has had any type of colorectal cancer screening, according to the Centers for Disease Control. The need for more screening is clear—but non-invasive tests that do not require anesthesia may become more popular as more health insurers offer coverage. Since October 2014 CMS has recognized stool-based DNA and fecal occult hemoglobin as covered services (as long as they are done by laboratories authorized by the manufacturer to perform the Cologuard™ test.) (See MLN Matters®Number: MM9115.) Although CMS does not currently cover computed tomography or “virtual” colonoscopies, that could change if a bill introduced in the U.S. Senate late last year—the "CT Colonography Screening for Colorectal Cancer Act of 2015,” S. 2262—were to be enacted into law.
The bill’s chances for passage are slim in the near future; one reason is that the U.S. Preventive Services Task Force (USPSTF) does not recommend CT colonoscopies because of lack of evidence of effectiveness and concerns about radiation exposure and false positives. The USPSTF guidelines do list virtual colonoscopies as an alternative screening option, however. Cancer Therapy Advisor quotes Judy Yee, MD, chair of the American College of Radiology Colon Cancer Committee stating that "Cigna, United Healthcare, Anthem Blue Cross Blue Shield, and other major insurers cover screening virtual colonoscopy. More than 20 states require insurers to cover these exams."
The attraction of virtual colonoscopies and other non-invasive colorectal cancer screening tools is their relative lack of discomfort. As the technologies improve and prove themselves, better insurance coverage will likely ensue.
In the shorter term, however, lower payment for colonoscopies may discourage enough gastroenterologists from performing these procedures on Medicare patients, which may in turn affect some anesthesia practices’ case mix and profitability. Commercial health plans may follow CMS’s lead and reduce their payments in turn. Representatives of the gastroenterology associations have pointed to such dire consequences as a shift of sites of service from efficient ASCs to less efficient hospital outpatient departments, practice mergers “to form supergroups that share operational costs,” “a massive migration from private practice into hospital employment/affiliation” and fewer new physicians choosing gastroenterology residencies. (Pallardy C. GI Society Roundtable: Putting Together the Game Plan for Potential Colonoscopy Cuts. Becker’s GI & Endoscopy, July 31, 2015.)
With Medicare payments for anesthesia for screening colonoscopies also on the chopping block, some of our readers should think about evaluating the role and delivery of these services in their mid- to long-range planning.
The past several years have, once again, brought major changes to the anesthesia community and have greatly impacted private practice anesthesia. Whereas the early nineties were a time of “anesthesia surplus” when anesthesiologists struggled to find opportunities paying as little as $100,000, those days were followed by a shortage of anesthesia providers. Supply and demand economics dictated that during the days of anesthesia staffing shortage, prices and compensation for anesthesia staff increased to the highest levels in history. Now, a new day is on the horizon where hospitals have many choices for anesthesia coverage. Smaller, private practice anesthesia groups struggle to sustain financial viability. Many groups are exploring mergers to achieve economies of scale and hoped-for negotiation leverage with private payers. Larger and mega-groups continue to liquidate their value and sell to publicly traded companies such as EmCare or MedNax. A growing number of large anesthesia staffing companies continue to enter the market. Daily, hospitals are approached by multiple anesthesia staffing providers in attempts to contract for a hospital’s anesthesia business; large, publicly traded companies offer hospitals the opportunity for “one-stop-shopping” for hospital-based physician services. In summary, this means increased competition among private anesthesia groups to retain their contracts with hospitals.
Image may be NSFW. Clik here to view.With hospitals under increased financial pressures and needing to focus on the bottom line, a group’s preaching to the hospital about quality care and loyalty is insufficient to retain its contract. The fastest way to encourage a hospital to seek an alternative anesthesia provider is for the group to request an increased stipend without demonstrating commensurate financial and service value to the hospital. The hospital is the anesthesia group’s client. Groups need to quickly understand and provide high levels of client service in order to retain their contracts.
In healthcare we speak a lot about “the customer” and providing “customer service”; many hospitals engage organizations such as Disney, Marriott and Studer to educate them about customer service. Alas, most of this customer service is of the “softer” kind and is really about “customer satisfaction” or what we typically refer to as “soft and fuzzy” and making the patient feel satisfied or valued. For anesthesia, this element of customer service needs to be understood and provided. The service must provide quantifiable, financial value, however, in addition to the historically intangible value of clinical quality. Pay for Performance tools assist in measuring the lack of, or deficits of, clinical quality, but not necessarily levels of exceptional clinical quality. What this means for your group is that the unwritten and unspoken expectation of performance is clinical service at an exceptional level. All too often anesthesia is heard to whine, “anesthesia gets no respect.” To this we reflect on “The Serenity Prayer” which states in part: Allow me to accept the things I cannot change and provide me the wisdom to change the things I can. Anesthesia groups need to accept the existing finances of healthcare reimbursement and focus on changing their hospital’s perception of them. Groups need to earn the respect of their hospital clients by providing and demonstrating measurable, financial value, which for anesthesia, extends well beyond the practice of good medicine. For the hospital, the operating room is the single greatest producer of revenue and typically accounts for at least 65 percent of hospital revenue and profit. Anesthesia groups need to reprogram their thinking and stop focusing on “how much money anesthesia and the OR make for the hospital,” and begin focusing on How Anesthesia Can Assist the Hospital to Make More Money!This is the primary way to demonstrate your group’s value and retain your contract!
Anesthesia’s ability to demonstrate value rests in four primary buckets:
Exceptional clinical outcomes – this is an expectation that seldom gets recognition; deficient outcomes get recognized and have associated financial penalties.
Development of new clinical service offerings (chronic pain management, etc.).
Assistance with improving perioperative program operational efficiencies, which is the foremost factor in:
Assistance in increasing case volume, which is the greatest revenue producer for the hospital and best enables anesthesia to demonstrate its value.
The remainder of this discussion focuses on anesthesia’s ability to assist in increasing OR case volume and associated revenue, by developing OR programs that are surgeon service oriented and make optimal use of surgeon time.
In the operating room we regard the surgeon as the customer. The surgeon wants to be seen as a patron of the hospital; the customer maintains the option to shop elsewhere. The hospital-business will not survive without the physician (and patient) customer(s). As in the retail environment the physician-customer maintains an expectation that the vendor (hospital) delivers a quality product. However, in the hospital setting, the product is a service vs. a tangible product; physician-customers place primary emphasis on the hospital meeting their service oriented expectations. Anesthesia is a driving force in meeting surgeons’ expectations which primarily are:
Quality patient care, which is taken for granted.
Experienced OR staff who can anticipate surgeon and case requirements, and also good equipment/instruments.
Sufficient OR access, in balance with surgeons’ practice needs, by hour of day and day of week. This requires staffing by OR and anesthesia.
Optimized/efficient use of surgeons’ time. This requires a collaborative effort, by all parties, including OR, anesthesia and the surgeon. Anesthesia needs to be the driver, or champion, of efficient perioperative services operations.
Image may be NSFW. Clik here to view.The reality is that anesthesiologists do not refer patients to hospitals. Anesthesiologists must pose a question to themselves: Do you consider yourself a consulting specialist, and if so, then, don’t consulting specialists need to garner referrals; don’t consulting specialists need to develop and protect referral sources? The surgeon is anesthesia’s referral base and anesthesia must assist the hospital to accommodate surgeons’ needs and expectations and to build case volume.
In general, customers’ expectations, regardless of who the customer is, will not be met unless expectations are reasonable and clearly defined. Most frequently, for anesthesia, this involves establishing how many anesthesia sites are staffed by hour of day and day of week. The number of staffed sites can not be a moving target if customer service is to be effectively delivered; however, anesthesia must be reasonably flexible to accommodate varying activity levels and must be service oriented. In addition to agreement on the number of staffed sites, in order for anesthesia to effectively provide customer service, anesthesia must be able to rely on:
An OR committee (or governance body) having developed effective scheduling policies and procedures and further, consistently enforcing them,
Surgeons’ offices effectively communicating with OR scheduling,
Surgeons effectively communicating with anesthesia with regard to difficult cases or sick patients,
Nursing effectively implementing preadmission screening protocols that have been developed jointly with anesthesia,
Charts being completed on the day of surgery,
Patients being appropriately prepared for surgery in either a preop unit or on the hospital floor,
Ability to transport the patient to the OR in a timely manner in order to have on-time case starts,
Surgeons reporting to the OR on time for on-time case starts,
Experienced OR staff and appropriately set-up cases in order to reduce case times,
Experienced charge nurses working with anesthesia to run the day’s schedule, and
Experienced PACU staff who can function with relative independence.
Image may be NSFW. Clik here to view.In turn, an effective anesthesia group, demonstrating value to its client hospital, will be providing services as outlined in the anesthesia contract and services agreement and will be measured and monitored on a regular basis through use of some type of score-card. Where anesthesia stipends are in place, a portion of the stipend should be placed at risk and evaluated based on mutually agreed “riskreward” criteria. The score-cards are used to measure anesthesia’s performance, to provide anesthesia financial incentives for good performance and to penalize deficient performance against the stipend. This is how anesthesia groups come to the negotiating table as true business partners of the hospital. Anesthesia groups need to provide at least the following elements of services value to their hospitals’ perioperative programs:
Be current in state-of-the art anesthesia care with an emphasis on ambulatory anesthesia,
Maintain reasonable flexibility with regard to agreed expectations—maintain an attitude of meeting or exceeding expectations,
Assure consistent and reliable staffing for all anesthesia sites agreed to,
Take ownership in developing and providing oversight for effective preadmission screening programs. Agree as a group to established guidelines and algorithms. Collaborate with nursing on the administration of the preadmission screening program and assist with nursing education,
Screen all ASA III and above patients and visit with all inpatients prior to the day of surgery. Develop processes to administer anesthesia consults for the preadmission unit. Call patients on the evening prior to surgery. Be as familiar as possible with patients’ conditions prior to the day of surgery,
Review patient charts at least the day prior to, if not several days prior to surgery,
Proactively work with nursing on schedule planning and management and proactively assist nursing to enforce scheduling policies. Assign a lead charge anesthesiologist to work with the charge nurse/OR Manager on schedule planning and daily schedule administration,
Begin reviewing the schedule with nursing several days prior to surgery,
Facilitate getting patients into the OR for on-time case starts,
Facilitate expediting turnaround time,
Where appropriate, maintain an effective medical direction model where CRNA direction is based on case complexity, patient acuity and CRNA skill level,
Be promptly available to CRNAs during on-going cases and also to CRNA cases to expedite induction and emergence,
Develop a staffing model and service agreement model whereby anesthesia staffing requirements of remote sites does not disrupt OR staffing,
Develop a quality improvement and education model for all anesthesiologists, CRNAs and hospital staff (RNs, RTs), where appropriate,
Assign lead individuals to foster skills and business development in key services such as cardiac/ vascular, OB, ambulatory, pain (and, potentially, neuro, trauma, pediatrics),
Focus on delivering the highest level of patient care with respect for the patient’s time and provide hospitality,
Focus on defining expectations and then exceeding those client/ customer expectations in efforts to assist the anesthesia practice to flourish,
Depending on expectations, payor mix and OR efficiencies and case times, there may still be a need to approach hospital administration for a stipend payment to deliver on expectations,
Play a key role in developing and sustaining your business/your practice by focusing on what is required to develop a marketable and financially viable surgical program with increasing case volume.
Image may be NSFW. Clik here to view.Indeed, all of the above will require a reinvented approach and mindset on the part of anesthesiologists in private practice. Providing increased value to your hospital client will require increased effort and time on the part of group members. The motivating factor must be the drive to remain in private practice as long as possible; to sustain the financial viability of your practice/business. Every business, regardless of its service offering or discipline, must continue to reinvent itself, to remain marketable, in changing times. Anesthesia is no exception. The group will incur increased expenses in providing these services to the hospital. The expense of losing your contract, however, is far greater.
Anesthesia Business Consultants (ABC), a leading provider in billing and practice management for the anesthesia and pain management specialty, is pleased to announce it will be attending PRACTICE MANAGEMENT 2016 hosted by the American Society of Anesthesiologists, held January 29-31 at the San Diego Hilton Bayfront in San Diego. This event is the premier business event for physician anesthesiologists and practice administrators.
ABC will be demonstrating its new anesthesia-specific ICD-10 documentation application, F1RSTCode. Unlike other apps in the industry that are not specialty-specific, F1RSTCode assists anesthesia providers in understanding documentation requirements without burdening them by requiring a search through the entire ICD-10 code sequence.
In a very logical and intuitive way, F1RSTCode takes you from the surgical procedure through the logic of ICD-10. It not only provides invaluable guidance for documenting the diagnosis, but will also provide a framework for discussing the post-operative diagnosis with the surgeon during the post-op time out.
PRACTICE MANAGEMENT 2016 is a perfect venue for presenting F1RSTCode. ABC is committed to the anesthesia industry and F1RSTCode is an application that is exclusively available to ABC's clients. F1RSTCode is the only anesthesia-specific application that targets anesthesia providers.
ABC is fully immersed in using data to benefit our clients, to enhance their ability to manage the practice side of their roles as anesthesia professionals. F1RSTCode, along with F1RSTAnalytics, our Big Data tool, enhances a practice’s operational performance, thereby enhancing its clinical excellence. Our clients want to work smarter and want to see demonstrable results.
F1RSTAnalytics works in tandem with ABC's proprietary software F1RSTAnesthesia, giving clients a powerful tool to convert clinical information into claims for reimbursement. The software supports electronic claims editing to ensure consistently high billing acceptance rates, and minimizes manual intervention in payment posting through direct remittance processing. Clients are able to access the details of their practice and to view trends securely online.
You can find ABC at Booth #408 of the San Diego Hilton Bayfront.
The Medicare requirement that eligible professionals and hospitals demonstrate “meaningful use” (MU) of electronic health record (EHR) technology has received a lot of attention from provider organizations and in the media recently. Two significant MU developments have occurred in the last few weeks: (1) the Centers for Medicare and Medicaid services (CMS) launched a streamlined process for claiming a hardship exemption and (2) CMS Acting Administrator Andy Slavitt stated publicly that the MU program “will now be effectively over and replaced with something better.”
Before explaining those two events, let us first assure readers that the MU program has not changed as far as its impact on anesthesiologists is concerned: all physicians with the specialty designation “anesthesiology” (“05”) in the Medicare Provider Enrollment Chain and Ownership System (PECOS) continue to benefit from an automatic exemption from the MU requirements. Let us remind you, too, that any physician who satisfies the MU requirements may still qualify for the incentive payment, and also that nurse anesthetists are not “eligible professionals” for purposes of the MU program.
Physicians with the PECOS designation “72” (pain management) or “09” (interventional pain management) who did not satisfy the MU requirements in 2015, however, may want to apply for a hardship exception and thus avoid penalties in 2017. Any “critical care/intensivist” with the PECOS code“81” who does not qualify for the exception for hospital-based physicians—those who provide 90 percent or more of their covered services in a hospital inpatient or emergency room setting—might also apply.
The simplified process for claiming the hardship exception came about as a result of the Patient Access and Medicare Protection Act (PAMPA), enacted in late December 2015. A provision in PAMPA granted CMS expanded authority to process meaningful use hardship exceptions for the 2015 performance year by category of provider rather than on a case-by-case basis. Organized medicine had lobbied for the change because of the delayed release of the 2015-2017 meaningful use modifications rule, which prevented many eligible professionals and hospitals from satisfying the MU requirements in 2015.
The deadline to submit the application for eligible professionals is March 15, 2016. The completed form can be emailed or faxed to CMS. (CMS will continue to accept hardship applications on a traditional case-by-case basis until July 1st.)
A single application can be submitted for multiple physicians in a group.
The information that must be provided includes the grounds for the exception. There are two exceptions under the heading “Extreme and Uncontrollable Circumstances” of particular interest:
Issues with the certification of the EHR product or products such as delays or decertification, issues with the implementation of the Certified EHR Technology (CEHRT) such as switching products, or issues related to insufficient time to make changes to the CEHRT to meet CMS regulatory requirements for reporting in 2015, and
Inability to control the availability of CEHRT at a location or locations constituting more than 50 percent of patient encounters.
“Inability to control the availability” of CEHRT might apply to physicians who are locked in to their hospitals’ or surgery centers’ EHRs. Other exceptions listed on the application are lack of internet connectivity, bankruptcy or closing of practice or hospital, lack of face-to-face patient interaction and natural disasters. All that is necessary is an attestation by the practice representative that the exception applies; details are not required.
In the past, CMS has granted more than 85 percent of case-by-case hardship applications.
The hardship exception will only cover the 2015 performance year and avert payment adjustments in 2017. The MU program is set to continue through 2018, however.
CMS Acting Administrator Slavitt caused a major stir when he said, at the J.P. Morgan Annual Health Care Conference on January 11th, that the MU program was “effectively over” and that it will be “replaced with something better.” The “something better” would be the EHR component of the Merit-Based Incentive Payment System (MIPS) created by the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA). MIPS will measure and compensate physicians on four distinct elements: quality, practice improvement, cost, and use of technology. Within MIPS will be elements of meaningful use. Rather than rewarding physicians for using technology, beginning in 2019 MIPS will aim to pay them for using it to improve their outcomes.
Slavitt’s comments were welcomed by many providers and Health Information Technology officers, who expressed relief at the eventual demise of the Byzantine, rigidly prescriptive MU program—the requirements of which are still changing. (Mace S. "Meaningful Use ‘Bombshell' Leaves Nary a Mark.” HealthLeaders Media online, January 19, 2016.) But MU Stage 2 is still in effect. In 2017, participation in Stage 3 will be optional, and in 2018 all providers are expected to implement Stage 3 certified EHR technology. (See ABC Alert dated October 26, 2015, CMS Releases Final Electronic Health Record Incentive Program Stage 3 Rules – Anesthesiologists Retain Exemption) The details of MIPS are a black box until CMS publishes proposed regulations, as it is expected to do this spring. Slavitt did not give any particulars on how and when CMS would organize the transition from MU to MIPS.
Within days, Slavitt made it clear that changes would take time, stating in a blog post: “We encourage you to look for the MACRA regulations this year; in the meantime, our existing regulations—including meaningful use Stage 3—are still in effect."
Thus the MIPS version of MU is due to be proposed in March or April and finalized before the end of this year. Payment adjustments in 2019, the first year of MIPS, will most likely be based on 2017 performance. As things stand now, physicians are apparently expected to begin meeting the MU requirements of MIPS in 2017—and then to implement Stage 3 of the earlier EHR incentive program in 2018. Anesthesiologists are automatically exempt from Stage 3—but will they be exempt from the MIPS requirements regarding the use of EHRs?
Does CMS even have the ability to decide to terminate the MU program early, given that its basis is in legislation passed by Congress?
Could it be more confusing?
“Clearly, CMS has a lot to work out. What is undeniable, though, is that the Stage 3 rule was finalized without consideration of the changes to Medicare mandated by MACRA. Now, the agency is trying to reconcile the two, with the Meaningful Use program not so gracefully bowing out.” (Commentary, “The Speech Heard Around the Healthcare Industry.” Health Data Management online, January 15, 2016.)
We hope that the reconciliation will be to our readers’ benefit.
One of the biggest takeaways from the ASA Practice Management Conference held in San Diego on January 29-31 was the need for anesthesiologists to start thinking about what the Medicare and CHIP Reauthorization Act of 2015 (MACRA) will mean for their practices.
Physicians are already benefiting from the MACRA provisions that repealed the Sustainable Growth Rate (SGR) formula that would have driven Medicare payments down dramatically had Congress not overridden it every year. Instead of a 27 percent SGR cut that would have been implemented on April 15, 2015 absent the legislation, payments increased by 0.5 percent on July 1st. They were to increase again by 0.5 percent on January 1st of this year but adjustments for budget neutrality and a target reduction for allegedly misvalued codes in each of the next three years caused them to decrease by 0.2 percent.
Beyond 2016, MACRA provides for 0.5-percent conversion factor increases in 2017-2019 and for 0 percent increases in 2020-2025. And beyond replacing the SGR with set percentage increases for a decade, MACRA will move professionals farther along the volume-to-value trajectory through payment adjustments for participation in either of two new programs: the Merit-Based Incentive Payment System (MIPS) and Alternative Payment Models (APMs).
MIPS
The MIPS will simplify and streamline Medicare's current quality reporting programs into a single payment-adjustment system beginning in 2019. The Physician Quality Reporting System (PQRS), the Value-Based Payment Modifier (VM) and the Meaningful Use (MU) program will all end in 2018. Physicians and other Eligible Professionals (EPs) will be evaluated through a Composite Performance Score (0-100 points) based on the four components in Figure 1 below:
Initially, in 2019, the EP’s MIPS Composite Performance Score will be weighted on the four components in the proportions shown in the first column in Table 1 below. By 2021, the proportions will shift:
Table 1. Components of the Composite Performance Score
Add Chart
The first three components are familiar. Some of the measures of “quality” will come from the PQRS and from Qualified Clinical Data Registries (QCDRs). New measures will build upon various sources including those for inpatient hospitals. “Resource Use” will require CMS to develop applicable cost measures and methods for attributing patients to different providers. (CMS does not currently have any way of attributing costs to anesthesiologists. As Stanley W. Stead, M.D., M.B.A. wrote in MACRA Strategy: Quality Reporting and Contribution to Savings in the July 2015 ASA Newsletter, “In cases where an EP cannot participate in a category, the law is unclear.”) CMS will develop a new definition of “Meaningful Use” of electronic health records. “Clinical Practice Improvement Activities” are a brand-new category that encompasses communication and patient safety measures such as:
Expanded practice access, such as same day appointments for urgent needs and after hours access to clinician advice
Population management, such as monitoring health conditions of individuals to provide timely healthcare interventions or participation in a qualified clinical data registry
Care coordination, such as timely communication of test results, timely exchange of clinical information to patients and other providers, and use of remote monitoring or telehealth
Beneficiary engagement, such as the establishment of care plans for individuals with complex care needs, beneficiary self-management assessment and training and using shared decision-making mechanisms
Patient safety and practice assessment, such as through use of clinical or surgical checklists and practice assessments related to maintaining certification
EPs’ composite scores will be compared to a performance threshold that will be set each year based on the mean or median of the MIPS scores for all EPs in a prior period as selected by CMS. Composite scores below the performance threshold will incur MIPS penalties and those above the threshold will generate variable bonuses, on a sliding scale, up to the maximums in Table 2:
Table 2. Maximum Positive and Negative MIPS Adjustments as a Percentage of Medicare Payments
Depending on individual performance, the adjustment may also be neutral. The dollar amounts of the upward adjustment will not be determined until CMS analyzes MIPS performance across all EPs, because by law the MIPS program must be budget neutral, with the losers paying for the winners’ gains—think Hunger Games. Bonuses could go even higher, up to three times the maximum penalty levels, but the total of the bonuses and penalties must essentially balance one another.
MACRA provides additional funding for separate bonuses of up to 10 percent for exceptional performance, up to $500 million per year, from 2019 through 2024. So even if all physicians score above the threshold, some will still receive incentive payments. Beginning in 2026, all EPs participating in MIPS will be eligible for a 0.25 percent increase in annual payments.
There are three groups of physicians and practitioners who will not be subject to MIPS:
Those in their first year of Medicare participation;
Those whose volume of Medicare patients is below the threshold, and
Participants in eligible APMs who qualify for the bonus payment.
APMs
The last type of Clinical Practice Improvement Activities on which MIPS scores will be based is “Participation in an alternative payment model.” EPs who receive a “significant portion” (Table 3) of their Medicare payments through an eligible APM entity, however, will be totally exempt from the MIPS requirements and will be “qualifying APM participants” (QPs). QPs will receive a five percent bonus in each of the five years between 2019 and 2024. From 2026 onward, they will be eligible for 0.75 percent increase in their annual Medicare payments—half a percent more than EPs who merely satisfy MIPS. CMS is clearly trying to encourage physicians to participate in developing new payment models that produce reductions in costs.
Table 3. “Significant portion” of Medicare payments required to qualify for APM bonus
add chart
MACRA identifies the following CMS programs as sources of eligible APM entities:
CMS Innovation Center (CMMI) model (other than a Health Care Innovation Award)
MSSP (Medicare Shared Savings Program), e.g., Accountable Care Organizations (ACOs)
Demonstration under the Health Care Quality Demonstration Program, e.g., Medicare Health Care Quality Demonstration Program or Medicare Acute Care Episode Demonstration Program
Demonstration “required by Federal Law”
To be an eligible APM, the above Medicare programs and any others that are to be approved must meet the following criteria:
Base payment on quality measures comparable to those in MIPS, and
Require use of certified EHR technology, and
Either (1) bear more than nominal financial risk for monetary losses or (2) be a medical home model expanded under CMMI authority.
Not much more is known about how APMs will be approved or how they will operate. CMS is expected to issue a proposed rule on the implementation of the APM and MIPS programs in March or April. There will then be a 60- or 90-day period for public comments to be submitted to CMS. CMS will consider the comments and then, late this year, publish a final rule with details of the MIPS measures and APM criteria. The first MIPS performance year, on which the 2019 adjustment will be based, will be 2017. The first measurement period for assessing whether EPs are QPs will be 2018 and the first incentive payments will be made in 2019. “ASA believes that a [Perioperative Surgical Home] is well positioned to become an APM,” Dr. Stead stated. We agree, and we will continue to share what we learn with our readers.
Being sued by a patient who had a poor outcome is one of the more unpleasant experiences most doctors can contemplate. The impact of a malpractice lawsuit can be potentially devastating to one’s financial, professional and personal well-being. But it is not often that bad. In a survey conducted by Medscape among 4,000 physicians (Peckham C. Medscape Malpractice Report 2015: Top Reasons Doctors Get Sued—Anesthesiologists. January 22, 2016), the responding anesthesiologists reported that trial resulted in a verdict for the plaintiff in only two percent of cases. Another 33 percent were dismissed either by the court or by the plaintiff. Twenty-four percent were dismissed from the suit either before any depositions were taken or within the first few months. Forty-one percent settled before reaching the verdict stage, and 10 percent resulted in a verdict in the anesthesiologist’s favor.
Malpractice litigation usually ends in the anesthesiologist’s favor or with a settlement that is considerably less than the amount of damages sought in the “complaint,” the document that launches the lawsuit. Most anesthesiologists will face a malpractice suit during their careers, nevertheless. Among the respondents to the Medscape survey, 62 percent of men and 42 percent of women had been sued, usually with other co-defendants. The reason for the gender-based difference may be that more male anesthesiologists have been in practice for longer periods of time; 100 percent of respondents aged 70 or older had been named in at least one lawsuit.
Anesthesiologists are more likely to be sued in the West (CA, HI, AK) and the Southeast (SC, GA, FL, AL, MS, TN, KY) and least likely in the Southwest (AZ, UT, CO, NM, NV).
Win or lose, being sued is going to cost the defendant anesthesiologist a lot of valuable time. Thirty-seven percent spent more than 40 hours preparing for trial. Thirty-six percent spent more than 50 hours in court. Fifty-nine percent of case lasted for 0-2 years, but 41 percent lasted three years or more.
The harm most commonly alleged was “patient suffered an abnormal injury (47 percent)” ranging from loss of life to dental damage. Failure to diagnose was second, at nine percent. Errors in medication administration and “poor documentation of patient instruction and education”—both are the subject of various active quality measures—tied at four percent.
Medscape references a 2011 JAMA study that “reported that 48 percent of paid claims were for events in inpatient settings, 43 percent in outpatient settings, and nine percent in both. Suits in the outpatient settings were more likely to be due to diagnostic issues and surgical errors were more often the cause in the inpatient setting.” (Bishop TF, Ryan AM, Casalino LP. Paid malpractice claims for adverse events in inpatient and outpatient settings. JAMA. 2011;305:2427-2431.) Those proportions were rather different over the nine year period (2005-2013) for which Richard J. Kelly, MD, JD, MPH, FCLM, an anesthesiologist from the University of California, Irvine School of Medicine, examined the change in outpatient anesthesia-related malpractice payments with a comparison of important inpatient and outpatient malpractice claim characteristics: payment size, patient demographics and clinical outcome, presenting his study as abstract A2097 at the 2015 ASA Annual Meeting. Overall spending on anesthesia-related claims, Dr. Kelly noted, had decreased by $83.3 million, or 41.4 percent.
Using National Practitioner Data Bank data, Dr. Kelly found that of the 2,408 payments made by anesthesiologists during the period studied, 567 (23.5 percent) were for outpatient events and 1,841 (76.5 percent) were for inpatient events. (Doyle C. Medical Malpractice Claims against Anesthesiologists Decrease and Shift to Outpatient Anesthesia Services. Anesthesiology News, December 7, 2015.) While the proportion of outpatient claims increased along with the number of cases being done in outpatient departments or surgery centers, the amounts paid for those outpatient claims remained significantly lower ($189,349 vs. $261,742).
If the number of anesthesia-related claims from inpatient procedures has been decreasing, another team of researchers led by Karen B. Domino, MD, MPH, professor of anesthesiology at the University of Washington, reported at the same ASA Annual Meeting (Abstract A1009) that they are more frequent than claims from events occurring in non-operating room (OR) locations—but that payments are both greater and more likely in non-OR claims than in those coming from the general OR. The non-OR cases in the study had a higher mortality rate as well. (Vlessides M. Claims Payments and Mortality Higher in Non-OR Settings. Anesthesiology News, November 3, 2015.)
Dr. Domino et al. compared anesthesia malpractice claims for events occurring in gastroenterology, cardiology and radiology procedure rooms between 2000-2012, that were reported to the Anesthesia Closed Claims Project, with the much larger National Anesthesia Clinical Outcomes Registry (NACOR) database.
Anesthesia care was more commonly assessed as substandard in non-OR claims (66 percent) than those from the general OR (44 percent; P=0.001). Payment was also more common in non-OR claims (72 percent vs. 57 percent; P=0.014) and were [sic] significantly greater (median $554,000 vs. $285,000; P=0.003).
Contributing to the substandard quality of the care in non-OR settings was the observed lack of properly-functioning pulse oximeters or end-title capnography monitors or advanced airway devices. The researchers “found that respiratory events were significantly more common in non-OR locations (53 percent vs. 23 percent; P<0.001). Inadequate ventilation or oxygenation occurred in one-third (31 percent) of non-OR claims. What’s more, in a full 35 percent of non-OR claims, the injury was deemed to be ‘possibly,’ ‘probably’ or ‘definitely’ preventable by better monitoring (compared with 17 percent in general OR claims; P=0.001).”
Thus the shift of surgical cases from general ORs to outpatient facilities appears to have been accomplished without any decrease in safety, which suggests appropriate selection of both patients and procedures for outpatient surgery, in addition to constantly improving technology. In contrast, the non-OR procedure rooms to which cases have migrated from the general OR have a relatively poorer track record, based in part on less reliable monitoring equipment and sometimes dark rooms with interruptions and other distractions that prevent the anesthesiologist from noticing that the patient has inadequate ventilation.
For various reasons—not least of which is the increasing age and fragility of many surgical patients—there will continue to be adverse outcomes and malpractice claims. Consider the advice of the Medscape survey respondents:
Image may be NSFW. Clik here to view.
As with much of the guidance presented in these eAlerts, we hope that you will not have occasion to use it—but if you do, you will know where to find it.
The Affordable Care Act requires Medicare physicians and others to report and return overpayments within 60 days after the date when an overpayment is identified. Four years after publishing its proposed rule, CMS issued a Final Rule on February 6, 2016 with the intent of providing “needed clarity and consistency for providers and suppliers on the actions they need to take to comply with requirements for reporting and returning of self-identified overpayments.”
Identification of an overpayment starts the clock for the repayment deadline of 60 days. The most significant point of clarification in the Rule is that “identification” of an overpayment occurs when “the person has, or should have through the exercise of reasonable diligence, determined that the person has received an overpayment and quantified the amount of the overpayment." Applying this principle may seem to require little explanation but CMS managed to spend nine pages discussing it in the Federal Register. It is also self-evident that often an attempt to reduce ambiguity ends up adding new ambiguities, and this final rule is one of those attempts.
A physician will typically be deemed to have acted with “reasonable diligence” if he or she conducts a “timely, good faith investigation” within “6 months from receipt of the credible information, except in extraordinary circumstances.” If the physician does not conduct such an investigation, lack of actual knowledge of the overpayment will not stand in the way of the enforceable obligation to repay the Government. The physician cannot rely on the “ostrich defense.” CMS specifies in its commentary that “If the requirement to report and return overpayments only applied to situations where providers or suppliers had actual knowledge of the existence of an overpayment, then these entities could easily avoid returning improperly received payments and the purpose of the section would be defeated.”
In addition, CMS uses its "reasonable diligence" standard to expand the provider's and supplier's obligations beyond merely investigating allegations of overpayments. Consistent with its position that the statute's requirement of repaying overpayments stands independently, CMS emphasizes in the preamble that "reasonable diligence" requires "proactive compliance activities" to identify overpayments, as well as reactive investigations into "credible information of a potential overpayment."
At the same time, however, expressly permitting the provider or supplier to conclude its "reasonable diligence" before an overpayment is deemed "identified" permits providers and suppliers additional time to conduct a factual investigation and then quantify any overpayment received, before the 60-day clock begins to run. For providers that do not exercise "reasonable diligence" when confronted with credible information of a potential overpayment, however, and that did receive overpayments, the repayment clock begins to run when they first receive that "credible information."
CMS provided a number of examples to help providers with understanding when an overpayment has been identified. The examples, “which were intended to be illustrative and not an exhaustive list of circumstances,” include the following:
A provider of services or supplier reviews billing or payment records and learns that it incorrectly coded certain services, resulting in increased reimbursement.
A provider of services or supplier performs an internal audit and discovers that overpayments exist.
A provider of services or supplier is informed by a government agency of an audit that discovered a potential overpayment, and the provider or supplier fails to make a reasonable inquiry.
Many observers welcomed a second major feature of the Final Rule, the look-back period, which CMS has now set at six years instead of the ten years indicated in the proposed rule. Thus overpayments must be reported and returned only if a person identifies the overpayment within six years of the date the overpayment was received. (We note that CMS’ instructions to the Medicare Administrative Contractors had long been that they could reopen claims only from the past 48 months for review of potential overpayments.)
CMS explained that a six-year rule would “appropriately address many of the concerns about burden and cost” raised by commenters on the ten-year proposal, since “many providers and suppliers retain records and claims data for between 6 and 7 years based on various existing federal and state requirements.” CMS did not make clear, however, whether the look-back period combined with the “reasonable diligence” requirement means that practices must conduct audits to determine whether there have been any overpayments in their six-year payment history. At least one commentator (the author of a blog entry on the Squire Sanders Boggs website entitled “CMS’s Final Overpayment Rule: What Providers and Suppliers Need to Know”) thinks that that interpretation is the correct one:
CMS appears to confirm this in commentary relating to the 6-year lookback, stating “[t]hus providers and suppliers have a clear duty to undertake proactive activities to determine if they have received an overpayment or risk potential liability for retaining such overpayment.” In light of this, the Final Rule’s administrative impact may be significant.
Lastly, the Final Rule addresses the methods for reporting and returning overpayments. It provides that providers and suppliers must use an applicable claims adjustment, credit balance, self-reported refund or another appropriate process to satisfy the obligation to report and return overpayments. This approach for returning overpayments provides an array of familiar options from which physicians and others can select.
Compliance with the new regulations explaining the requirement is important because physicians who do not meet the 60-day deadline could be subject to False Claims Act or Civil Monetary Penalties Law liability (treble damages plus $11,000 per claim, civil monetary penalties, and exclusion from the Medicare and Medicaid programs). CMS stresses that all providers and suppliers are subject to the statutory requirements of the ACA and could face potential liability even if the conduct falls outside the scope of the Final Rule. The Rule goes into effect on March 14, 2016.
“Ransomware” attacks are malicious intrusions into information systems that encrypt the victim’s sensitive data and demand payment in exchange for a key to unlock the data. They have become increasingly common in the last few years. Since January 2013, there have been at least 100,000 cases of recorded ransomware attacks.
The installation of such malware on third parties’ computer systems is usually paired with a demand for payment by a certain deadline or the computer data will be deleted. This is a more direct means for criminals to realize profits from hacking into hospital systems than selling medical records. It is also a more immediate, direct threat to patient welfare.
On February 5, 2016, Hollywood Presbyterian Medical Center in Los Angeles became one of the latest and highest-profile victims, demonstrating that “ransomware should be a permanent concern for anyone or any business using the internet, and it’s going to get worse before it gets better.” (Stone J. Ransomware Hackers A Bigger Threat Than Ever, Forcing Hospitals And Police To Pay Hostage Fees. IBT, February 23, 201.) Hollywood Presbyterian quickly paid the ransom of 40 bitcoins or about $17,000 (not $3.4 million as was initially reported) and finally, on February 15th, restored its electronic medical record (EMR) system. (Public letter from Allen Stefanek, Hollywood Presbyterian Medical Center President and CEO, February 17, 2016.)
During the ten days that the hospital’s computer systems were down, the staff was forced to revert to manual documentation using pen and paper to take down patient information and to jammed fax lines and telephones to communicate from one department to another. Patients were diverted to other facilities. Some outpatients missed treatments and others resorted to driving around town to pick up test results and other medical documentation that would normally be delivered electronically. It is unknown how many patients’ records or what types of information were affected, or if staff records and personal information were accessed.
Anesthesiologists and other hospital-based physicians who use the hospitals’ Information Management Systems (IMS) are just as vulnerable as the institutions themselves, and have considerable interest in encouraging the administration to make sure it is doing all it can to protect against ransomware attacks. Anesthesia groups running their own AIMS—and anesthesiologists who use smartphones; in 2014, four of the top five malware programs encountered by Android users in the United States were ransomware, posing as a legitimate app and then, after installation, locking the phone and demanding payment—should take their own preventive measures. Some of these are described below.
Actions Hospitals and Anesthesia Practices Can Take to Prevent a Malware Attack
As Stone says, “The best way to avoid an infection is to plan on being infected anyway. The only catch-all way to mitigate the damage is regular data backups, in the form of either cloud storage or a physical hard drive.” When a criminal then wipes all the data in the computer system, another up-to-date copy can be restored quickly. That is the single most important and most effective strategy to protect against a ransom demand.
Hospitals or practices that are doing backups on site should make sure they can recover an image of the data for months in the past and keep multiple copies. Any backups made between the time of infection and when the attack is detected will be encrypted, and thus unrecoverable without paying the ransom. For that reason, online backups with automatic incremental backups can be very useful. At the very least, providers should be keeping at least one set of backups offsite.
Mark Dill, a consultant at tw-Security and former Chief Information Security Officer at the Cleveland Clinic, encourages organizations to use a “People, Process and Technology” approach including the following steps, as described in 10 Steps to Reduce Your Ransomware Risks on the Health Data Management website:
Educate the workforce to be suspicious of and to resist clicking on links embedded in email or on a website while surfing the internet.
Ban all personal webmail and surfing on corporate devices. Make staff who bring their own mobile devices to work use those devices connected through a “guest” wireless network, to protect the internal network.
Implement a data backup plan with a longer retention schedule. Retain at least two months worth of full disk backups. Require staff to store all work-related data on a network drive rather than on a local or personal hard drive.
Create incident response procedures. Establish specific procedures and playbooks to address the most common types of attacks, and keep them updated. The first 48 hours after an attack are critical.
Filter internet traffic more closely. Consider restricting inbound and outbound internet traffic by creating a blacklist and/or a whitelist. Block inbound email traffic that comes from newly created domains, since hackers typically are using domains that are less than 72 hours old to launch their phishing attacks.
Review access rights on network drives. Only those employees who need to be able to write data to the hard drive should have access other than “read only.” “Least privilege” is a venerable information security principle.
Consider next-generation anti-malware tools that use advanced math to predict malware. The older antivirus solutions rely on pattern file updates and they are struggling to keep up with recent threats such as ransomware. You should also keep a pop-up blocker running in your web browser.
Evaluate advanced persistent threat (APT) tools. Many variants of the original and most successful ransomware start with an initial infection that requires them to access a Command and Control server on the internet to get the key that will encrypt the victim’s data. APT can see and block this communication and prevent the encryption.
Implement intrusion prevention systems (IPS). These function like APT tools by blocking the communication to the Command and Control server.
Patch vulnerable versions of PDF viewers and Flash players. Maintain software patches and make sure your operating system and all your applications are all up to date so no vulnerability can be exploited in order to deliver malware to your computers.
The number of cyberattacks, unfortunately, continues to grow. Last year in the U.S. more than 111 million individuals' data were breached due to a hack or IT incident, according to the Bitglass 2016 Healthcare Breach Report, cited by Becker’s Health IT & CIO Review in Large-scale cyberattacks account for 98% of breached health records (January 27, 2016). The article quotes the CEO of Bitglass as saying “As the IoT [Internet of Things] revolution compounds the problem with real-time patient data, healthcare organizations must embrace innovative data security technologies to meet security and compliance requirements.” Individual physicians and healthcare personnel, practice groups and healthcare systems must all make the necessary investments in cybersecurity.
We all know that the healthcare industry is experiencing a wave of integration. This trend has been evident for many years. Fewer physicians are willing to assume the legal, financial and other business risks associated with owning their own practices. More and more physicians, including anesthesiologists, are becoming employed by large physician groups, health systems and national providers.
Image may be NSFW. Clik here to view.This shift necessarily involves not only entry into new employment arrangements but also the termination of existing relationships. And those terminations are often governed by written employment agreements, state and federal healthcare laws and employer benefit plans and other policies and procedures.
Before pursuing their next opportunity, physicians should pause for a moment and first attend to the arrangement that they are leaving. Departing physicians need to understand their legal rights and obligations when leaving their current employment relationships in order to avoid unintended consequences and detrimental missteps along the way. Here are a few words of practical advice for physicians contemplating an exit from their current employment arrangements.
Ensure that the relationship is terminated in accordance with the terms of the written employment agreement. Whether the physician is terminating the employment agreement with or without cause, the physician is facing an involuntary termination initiated by the employer or the parties are mutually agreeing to end the relationship, the parties must terminate the relationship in accordance with the timing, prior notice and other procedural requirements set forth in the written employment agreement, when applicable. Failure to do so can result in a breach of contract claim and sometimes significant liability exposure.
Avoid relying on verbal promises and assurances regarding the transition. In the event that the parties have mutually agreed to terminate an employment relationship in a manner that is contrary to the terms of the written contract, such agreement should be reduced to writing. Verbal promises and assurances provided by the other party that it will cooperate and agree to waive certain rights under the employment agreement are generally not enforceable unless reduced to writing. Relying upon verbal promises and assurances is especially dangerous when the departing physician’s primary contact is not the ultimate decision maker and lacks ultimate authority to ensure a smooth transition.
Understand your obligations to obtain tail coverage. Employment agreements that permit professional liability insurance to be maintained on a claims made basis often require the physician (at least under certain circumstances) to assume the cost of obtaining tail coverage upon termination of the relationship. Before exiting an employment relationship, the physician should assess whether such obligation is present and the associated expenses. Note that the cost of tail coverage may vary greatly depending upon the particular state. Sometimes a physician’s obligation to procure tail coverage can be addressed, upon consent of the employer through an amendment to the written employment agreement, through the maintenance of the existing policy or by obtaining nose coverage.
Determine your rights and obligations to provide patients with notice of your departure. The right of a physician to inform his/ her patients of the departure is often addressed in the underlying written employment agreement. Many state laws also include provisions related to patient notices upon a physician’s departure. Non-solicitation provisions set forth within employment agreements are subject to applicable state law. Further, even when employment agreements include non-solicitation provisions and the state laws are silent on patient notices, physicians are sometimes able to persuade their employers to permit appropriate notices to patients based upon applicable ethical rules, principles of patient choice and continuity of care considerations.
Assume that noncompetition covenants will be enforced when permitted under applicable state law. It is common for physicians contemplating a departure to express disbelief that their employers would actually want to enforce a restrictive covenant or that a court would compel compliance with such an obligation. But they are often surprised. Employers place non-competes in their agreements for a reason—they believe they are important. When enforceable under applicable state law, non-competition prohibitions may significantly impact a physician’s post-termination career and should be taken very seriously. Physicians should review the restrictions carefully and objectively to ensure complete compliance. Applicable case law often informs how courts will interpret ambiguities within the contractual language (e.g., how the restricted geographic area would be determined). That being said, employers will sometimes grant waivers of such covenants when there is an incentive to do so.
Consider a separation agreement. In the event that either party has potential claims against the other or there are ambiguities in the underlying written employment agreement regarding the terms of departure, it may be best to enter a separation agreement. Whether a separation agreement is necessary or appropriate depends upon the particular circumstances and each party’s respective negotiating leverage. Separation agreements often include releases of claims and confidentiality, non-disparagement and indemnification provisions. They also often include, for example, provisions related to posttermination access to patient and billing records (for continuing care of patients, audits, litigation, etc.), non-solicitation and non-competition prohibitions, obligations to obtain and pay for tail coverage, the calculation and payment of bonus compensation, payout for unused vacation or sick time, settlement amounts and buy-outs, references provided by the employer to third-parties with respect to the departing employee and reports to licensure bodies, the National Practitioner Data Bank and governmental bodies, as applicable.
Anticipate collateral consequences, when applicable. Departing physicians should understand the impact that their employment termination may have on any medical staff memberships and faculty appointments. Also, those physicians who participate in or own the employing practice or related or third party physician organizations, accountable care organizations, co-management companies, ambulatory surgical centers, real estate investment entities and other ventures may need to terminate such membership or ownership interests in connection with the termination. Such termination requirements may be set forth in the employment agreement itself or in the shareholder, operating, participation or buy-sell agreements, as applicable.
Refrain from saying or doing something you regret. Some employment terminations are amicable but others are more like a bitter divorce. In such cases, it is often wise for physicians to take the emotion out of all negotiations and communications with the soon to be former employer and others to the extent possible and rely upon attorneys and other advisors to negotiate the transition when helpful. Employment agreements often contain confidentiality and non-disparagement provisions that apply during and after the term. Even when those requirements are not reduced to writing, physician employees should understand that they are generally not entitled to retain any property, passwords or confidential information of the employer after the termination. Further, even if the governing employment agreement does not include a nondisparagement provision, departing physicians should be careful not to impermissibly defame their employers or violate any applicable fiduciary duties owed to the employer on the way out as such actions can result in substantial legal exposure and financial liability.
Briefly stated, physicians should exit their existing employment relationships with care. It is advisable for physicians to take some time to review the terms of their written employment and related agreements, to understand their rights and obligations under applicable laws (including for example those pertaining to post-termination restrictive covenants, access to records and patient notices) and to understand how employer benefit plans will impact their departure. Before succumbing to the relief, hope, excitement (and perhaps even fear or anger depending upon the circumstances) regarding the termination and what lies ahead, physicians should take a moment to tie up any loose ends before moving forward.
"The intent of the guideline is to provide evidence-based recommendations for better management of postoperative pain, and the target audience is all clinicians who manage pain resulting from surgery," said principal author Roger Chou, MD of the Departments of Medicine and Medical Informatics and Clinical Epidemiology, Oregon Health and Science University, Pacific Northwest Evidence Based Practice Center. (APS News Release, February 17, 2016.) Studies have shown again and again that the majority of surgical patients receive inadequate pain control, which can increase the risks of persistent postoperative pain and of post-surgical complications, function and functional recovery, and quality of life.
The key recommendation in the Guidelines is for greater use of multimodal pain management strategies. Multimodal techniques, according to Dr. Chou, help achieve better pain relief while lowering doses of opioids and potentially avoiding certain adverse effects, by affecting pain through different pathways and mechanisms of action. Dr. Chou further explained that using a multimodal approach “means using different medications, for example opioids and nonopioid therapies such as non-steroidal anti-inflammatories (NSAIDs), gabapentin/pregabalin, ketamine, lidocaine, administered in different ways, for example, systemically or via neuraxial/peripheral regional anesthetic techniques, as well as medications and nonpharmacological therapies."
The Guidelines contain 32 recommendations developed by a panel of 23 experts in anesthesia, pain medicine, surgery, obstetrics and gynecology, pediatrics, hospital medicine, nursing, primary care, physical therapy and psychology who reviewed nearly 1,000 primary studies and systematic reviews. Although the process required only a two-thirds majority for a recommendation to be approved, unanimity or a near-unanimous consensus was achieved in each case.
Each recommendation received a separate grade for the strength of the recommendation (strong or weak) and for the quality of evidence (high, moderate, or low). Four recommendations received the highest ratings in both domains (strong recommendation, high-quality evidence):
Clinicians should offer multimodal analgesia, or the use of a variety of analgesic medications and techniques combined with nonpharmacological interventions, for the treatment of postoperative pain in children and adults.
Adults and children can be given acetaminophen and/or non-steroidal anti-inflammatory drugs as part of multimodal analgesia for management of postoperative pain.
Clinicians should consider surgical site-specific peripheral regional anesthetic techniques with proven efficacy in adults and children for certain procedures.
Spinal analgesia is appropriate for major thoracic and abdominal procedures, particularly in patients at risk for cardiac and pulmonary complications or prolonged intestinal distress.
The following recommendations are among those also rated “strong” albeit based on “moderate” quality evidence:
Oral administration of opioids is preferred to intravenous administration for post-operative analgesia.
Intravenous patient-controlled analgesia (PCA) can be used when parenteral administration of analgesics is required.
Clinicians should consider giving preoperative doses of celecoxib in adult patients without contraindications.
Gabapentin and pregabalin can be considered for multimodal postoperative analgesia. The medications are associated with lower opioid requirements after surgery.
Do not use routine basal infusion of opioids with IV PCA in opioid-naive adults.
Avoid intrapleural analgesia with local anesthetics for pain control after thoracic surgery.
Use continuous, local anesthetic-based peripheral regional analgesic techniques when the need for analgesia is likely to exceed the duration of effect of a single injection.
Avoid the neuraxial administration of magnesium, benzodiazepines, neostigmine, tramadol, and ketamine.
Avoid using the intramuscular route for the administration of analgesics for the management of postoperative pain.
The panel issued a third group of strong recommendations despite “low” quality evidence, including:
Clinicians should provide patient and family-centered, individually tailored education to patients and caregivers about treatment options for postoperative pain.
Every surgical patient should receive a preoperative evaluation, including assessment of medical and psychiatric comorbidities, concomitant medications, history of chronic pain, and substance abuse.
The pain management plan should be adjusted according to the adequacy of pain relief and the presence of adverse events.
Use a validated pain assessment tool to track response to postoperative pain treatments and adjust treatment plans accordingly.
Monitor sedation, respiratory status, and other adverse events in patients who receive systemic opioids.
Provide appropriate monitoring of patients who have received neuraxial interventions for perioperative analgesia.
Facilities in which surgery is performed provide clinicians with access to consultation with a pain specialist for patients with inadequately controlled postoperative pain or at high risk of inadequately controlled postoperative pain (e.g., opioid-tolerant, history of substance abuse).
Some of the recommendations were “weak” even if supported by moderate evidence. Among these recommendations were:
“The panel does not recommend routine use of local anesthetic infiltration. Rather, use of local anesthetic infiltration should be on the basis of evidence showing benefit for the surgical procedure in question.”
Clinicians should consider transcutaneous electrical nerve stimulation (TENS) as an adjunct to other postoperative pain treatments.
Clinicians should consider the use of cognitive-behavioral modalities in adults as part of a multimodal approach, e.g., guided imagery and other relaxation methods, hypnosis and intraoperative suggestions “(which involve positive suggestions to patients, usually under anesthesia, about the patient’s ability to manage and cope with postoperative pain and recovery from surgery)” and music.
Finally, the panel found itself unable either to recommend or to discourage acupuncture, massage, or cold therapy as adjuncts to other postoperative pain treatments because of insufficient evidence. The panel concluded by noting that there remain numerous research gaps. Of 32 recommendations, the panel rated only four as supported by high-quality evidence, and 11 recommendations were based on low-quality evidence
What impact will the new Guidelines have? They are intended, as noted above, to help physicians and other clinicians achieve optimal pain management following surgery. Given the intense health policy emphasis on the management of pain in general, hospitals may actively promote adherence to the Guidelines, which affirm the 2012 ASA Practice Guidelines’ recommendation that:
Whenever possible, anesthesiologists should use multimodal pain management therapy. Central regional blockade with local anesthetics should be considered. Unless contraindicated, patients should receive an around-the-clock regimen of COXIBs, NSAIDs, or acetaminophen. Dosing regimens should be administered to optimize efficacy while minimizing the risk of adverse events. The choice of medication, dose, route, and duration of therapy should be individualized.
Any changes in clinical practice that the APS Guidelines may bring about are likely to occur over time. Any changes in payment policies, such as requiring documented consideration of oral pain medications and relaxation therapy before administration of neural blockade, will come about slowly if at all—but anesthesiologists should certainly recognize that changes are possible and begin to update their own practices as appropriate.
When you received your 2016 Current Procedural Terminology (CPT) and American Society of Anesthesiologists (ASA) Relative Value Guide (RVG) books or discs, you probably noticed there were no new anesthesia code additions or deletions listed for this year. Since the CPT book usually arrives before the RVG, you may not have taken a good look through your RVG or may not have ordered a 2016 RVG as there were no coding changes. However, there are a number of important updates in the RVG New/ Revised RVG Coding Comments section which are not included in the Anesthesia section of the CPT. These comments may affect the way anesthesia coders assign procedure codes in the upcoming year. As this article will not include all updated comments, be sure to order your 2016 RVG. I’ve chosen a few that are certain to have an impact on 2016 coding for anesthesia services.
Let’s start with 00218, “Anesthesia for intracranial procedures; procedures in the sitting position” with a base value of thirteen units. As you may know, base unit values increase as the difficulty of a procedure increases. The new coding comment indicates “This code may be reported for anesthesia for any intracranial procedure performed with the patient in the sitting position.” For example, although the sitting position for cranial surgery is associated with a high incidence of air embolism (Schubert), a craniotomy or craniectomy for evacuation of a subdural infratentorial hematoma may be performed with a patient in the sitting position. Rather than assigning 00210 “Anesthesia for craniotomy or craniectomy for evacuation of hematoma” with a base unit value of ten, coders will assign 00218. This code assignment also depends on the anesthesia provider clearly indicating on the anesthesia record that the patient was in the sitting position.
Image may be NSFW. Clik here to view.Coders cannot capture billable services that are not indicated on the anesthesia record, even if they are marked on an internal billing sheet. Billing sheets are not usually considered as part of the patient’s medical records. There is no universal anesthesia record and a typical anesthesia billing company sees a number of different records, so coders must determine where on each record anesthesia providers document special positioning, which can be quite challenging with paper records and handwritten notes. With a paper record, the clearest way to document is a legible note in the remarks or comments section. Electronic anesthesia records (EARs) are much easier to read and may have a field summary, which typically includes an area to document when the patient is in the sitting, or any other special position. If the EAR doesn’t have a field summary, look within the body or comments section. If you are not sure where this information is documented, learn where patient positioning information is documented in your practice.
There were substantial changes to pacemaker coding comments under CPT codes 00530, 00534 and 00537 (See Table 1). The comments describe anesthesia for pacemaker services and indicate when it is acceptable to report the higher base unit values for active testing of an implantable cardioverter defibrillator (ICD) device or electrophysiologic (EP) testing. So it is important that (1) coders understand the difference, and (2) anesthesia providers are giving enough information to the coders to allow proper anesthesia code selection.
If cardioversion or defibrillator functions are not tested, coders are referred to CPT 00530, with a base value of four units. Documented testing of cardioversion or defibrillator functions increases the base value to seven units and is reported with CPT 00534. If an EP procedure is performed, CPT 00537 with a base unit value of ten is the appropriate anesthesia code. Coders should review these codes and circumstances with providers to ensure documentation supports the anesthesia code selected and reported, and be aware the Center for Medicare and Medicaid Services (CMS) has assigned a lower unit value than the RVG for EP procedures (See Table 1). The anesthesia codes for pacemaker related services are not listed in the MLN Matters article “National Coverage Determination (NCD) for Single Chamber and Dual Chamber Permanent Cardiac Pacemakers” (Number MM9078) as requiring a -KX modifier (indicating “Requirements specified in the medical policy have been met”) for Medicare patients, although the surgeon may be required to report a -KX modifier.
Another common area of interest to anesthesia coders is related to extracorporeal shock wave lithotripsy (ESWL). When I first started in anesthesia more than 32 years ago, it was common to see treatment for lithotripsy while the patient was immersed in a water bath; however, now it may be more common to see other types of ESWL treatment. According to Dr. Grasso, “In first-generation lithotriptors (Dornier HM3), the patient was placed in a water bath. However, with second- and thirdgeneration lithotriptors, small waterfilled drums or cushions with a silicone membrane are used instead of large water baths to provide air-free contact with the patient’s skin.” The 2016 comment for CPT 00872 indicates, “Use only when patient immersed in water bath. With small water filled drums/cushions, see 00873.” As there is a base unit value difference of two units between these codes, coders should ensure they are reporting as instructed. If you are not certain whether your practice’s facilities still use water bath or not, it’s time to check!
Image may be NSFW. Clik here to view.
CPT codes 36221–36626 describe non-selective and selective arterial catheter placement and diagnostic imaging of the aortic, arch, carotid and vertebral arteries. The 2016 ASA Crosswalk revises the reported anesthesia code for each of these procedures to 01916, “Anesthesia for diagnostic arteriography/venography” with a base value of five units. This is a substantial change from 2015 crosswalk codes ranging from six to ten base units.
Aside from multiple valuable comment and crosswalk code revisions, it is noteworthy that the 2016 RVG no longer includes ASA standards and guidelines relevant to coding and billing in the back of the book. The bad news is that it is no longer a matter of flipping through to the end of the RVG to access information when coders need to provide “proof” of why we do the things we do. The good news is the ASA provides all current version of their standards and guidelines on the ASA website (See Resources). While the information is not as convenient, unless you have internet access, keep in mind there is added value to having access to the most up-to-date information ASA provides.
Image may be NSFW. Clik here to view.Trying to keep up with ongoing changes to the Physician Quality Reporting System (PQRS) coding is a constant challenge for coders. There were no changes to the 2016 requirements for reporting cross-cutting measures, although a number of new cross-cutting measures have been added. However, PQRS coding is a different story.
You may have noticed in CPT Appendix B – Summary of Additions, Deletions and Revisions that there were textual changes to Category II Code 6030F (removing “cap and mask and sterile gown and sterile gloves and a large sterile sheet and 2 percent chlorhexidine” from the code description), and there were no Category II code deletions—but that doesn’t mean anesthesia coders don’t have to worry about deleted PQRS codes. Although Measure #44 (Category II Code 4115F) is still listed as a valid code, CMS removed this measure from claimsbased reporting. Code 4115F is still a valid code for registry reporting along with CPT 00562. In a nutshell, effective January 1, 2016, Measure #44 is no longer reportable if your anesthesia practice is using claims-based PQRS reporting.
Similarly, although Category II Codes 4250F and 4255F (Measure #193) are both still listed in the 2016 CPT, 2015 will be the last reporting year for this measure. Measure #193 has been retired and, it too, will no longer be reportable effective January 1, 2016. These changes, announced in the final physician fee schedule rule, which was published in the Federal Register on November 16, 2015, leave claims-based reporting anesthesia groups (estimated at 80 percent) only one PQRS measure specific to anesthesia – Measure #76 (Category II Code 6030F). Since anesthesia providers do not have nine measures across three domains, they will automatically be subject to the Measures Applicability Validation (MAV) process (unless they make a measure applicable to themselves by reporting it even once “unsuccessfully,” e.g., by appending the -8P modifier that shows that the measure wasn’t performed and doesn’t indicate that there was a valid reason for the non-performance. Many anesthesiologists unfortunately fell into this trap, which deems them to have failed PQRS altogether, for payment year 2016 based on 2104 reporting.)
The MAV applies to both claims-based and registry-based reporting, though the methodology differs. With claims-based, as there is only one applicable anesthesia measure (#76), as long as your provider meets the 50 percent threshold and also reports at least one “cross-cutting measure” if any apply (see below), no penalty should be assessed. Keep in mind that a claim with an -8P modifier, which indicates the action was not performed and no reason was documented, does not count toward the 50 percent threshold—or successful performance. Surprisingly, many anesthesia providers who successfully performed and reported PQRS in 2014 received a 2016 penalty notice (based on a two year look back period) and it appears other specialties experienced the same issue. Fortunately, the American Medical Association (AMA), Medical Group Management Association (MGMA) and the ASA are aware of the problem and are working toward a potential solution.
Unfortunately, anesthesia practices that do not place Swan Ganz or Central Venous Pressure (CVP) lines have no associated claims-based PQRS measures. According to the PQRS help desk (Quality Net communication to author), “if you are not able to report Measure #76 via claims, you are required to hire a registry for reporting the other applicable measures or a Qualified Clinical Data Registry (QCDR).” Although claims-based reporting of PQRS measures has not gone away, if you can’t report the only anesthesia PQRS measure left, registry reporting allows your anesthesia practice to report enough anesthesia specific performance measures to avoid payment penalties in 2018.
Similar to Measure #193, many of the registry-related PQRS codes include “G” codes as listed in the Healthcare Common Procedure Coding System (HCPCS) book. In 2016, there are no longer anesthesia clusters related to claims-based reporting. Cluster Number 38, Anesthesiology Care (for Registry-Based Measures), includes Measures #424, #426, #427 and #428 (See Table 2).
Image may be NSFW. Clik here to view.
Also, take a few minutes to thumb through the Category II performance measure codes listed in the 2016 CPT. The ASA has been working on developing specific measures relative to quality reporting of anesthesia services (see superscript number 11 under Category II footnotes). Many of these codes appeared in the 2014 CPT and several may look familiar to anesthesia coders. Codes listed in Table 3 are Category II performance measure codes developed by the ASA, although these codes are reported only through a registry.
By 2019, coders will see PQRS segue into a new quality program called the Merit-Based Incentive Payment System (MIPS). Whether you are a seasoned coder or new to the specialty, anesthesia coding will continue to be unique, interesting and challenging!
Image may be NSFW. Clik here to view.
Resources 2016 Professional Edition CPT American Medical Association
2016 Relative Value Guide and Crosswalk, American Society of Anesthesiologist
Donald Berwick, MD, senior fellow at the Institute for Healthcare Improvement (IHI) (and a former CMS administrator) described nine steps to advance healthcare into “the moral era” at an IHI forum in December, 2015. One of those steps was to “stop excessive measurement.” Dr. Berwick said:
I don’t mean that we should stop measuring. Indeed, I celebrate transparency in every form. How else can you learn? But we need to tame measurement. It has gone crazy. Far from showing us our way, these searchlights training on us, they blind us. ... I vote for a 50 percent reduction in all metrics currently being used.
Many anesthesiologists and pain physicians will agree that quality measurement has gone over the edge. The ASA’s Anesthesia Quality Institute (AQI) has adopted 22 measures and has identified 26 official Physician Quality Reporting System (PQRS) measures that can be reported by anesthesiologists and/or pain physicians. In proposing 48 distinct measures to CMS for use in its Qualified Clinical Data Registry (QCDR) in 2016—CMS’s approval is still pending—the AQI was obviously trying to provide an adequate selection for any of its members to be able to report the PQRS-required minimum of nine measures. But choosing the best measures for an individual practice is itself not easy and takes time. To begin with, there is the question of which type of measures the practice should focus on. Does it choose those that are the least demanding to report, or those that are the most meaningful for potential quality improvement?
The fact that the question of ease of reporting vs. worthiness of measures persists is an indication of the immature yet highly complex state of quality measurement. To put it another way, anesthesiologists and other physicians often ask, “How is all this helping patient care?”
The average physician spends 2.6 hours per week dealing with quality measures and their clinical and administrative staff spends another 12.5 hours per physician per week.
The combined total of 15.1 hours per week from paragraph 1 amounts to 785.2 physician and staff hours per physician per week.
The time spent by physicians and staff translates to an average cost of $40,069 per physician per year, or $19,494 in physician time alone. Annualized, the average cost for both physician and staff comes to $15.4 billion for just the four specialties surveyed.
Of the 394 practices responding to the survey, 81 percent reported that they spent more or much more effort dealing with external quality measures than three years ago.
Only 27 percent believed that current measures were moderately or very representative of the quality of care.
Only 28 percent used quality scores as the basis for quality improvement activities.
Data entry is by far the most time-consuming of the five elements surveyed, and the amount of time spent by the physicians in the four specialties varies considerably. The following table appears as Exhibit 6 in the Health Affairs article:
Image may be NSFW. Clik here to view.
A majority of the respondents wrote comments in the free-text portion of the survey instrument. “Five major themes recurred,” according to the authors: “the burden of current measurement requirements on small practices, recommendations to have measures that are uniform across entities, the need for specialty specific measures, the need for measures that better represent quality, and the need to easily and accurately extract data from electronic health records (EHRs).”
Many anesthesiologists and pain physicians would add a sixth theme: the inability of current quality measures to account for differences among patients, i.e., the lack of adjustment for severity of illness.
The survey conducted by Dr. Casolino and his team was one of the first formal studies of the burden of complying with externally-required quality measurement systems (not that it did not have limitations such as the possible overrepresentation of respondents who were dissatisfied). There has been a good deal of anecdotal criticism of the state of quality measurement in general.
The profusion of measures, questions about their validity and the EHRs that should be facilitating rather than impeding reporting together have contributed perhaps more than any other factors to a 50 percent burnout rate among physicians. (See Wachter RM. How Measurement Fails Doctors and Teachers. New York Times Sunday Review, January 16, 2016.) Casolino noted a “study of twenty-three health insurers [that] found that 546 provider quality measures were used, few of which matched across insurers or with the 1,700 measures used by federal agencies.” Different rules between Medicare, private payers and health systems as to the details required in reporting what is essentially a single measure increase the burden by orders of magnitude.
Fatigue is growing as performance on the various measures becomes increasingly linked to financial rewards and penalties. The PQRS, Value-Based Payment Modifier and the “Meaningful Use” of EHR technology incentive program have become complicated almost beyond comprehension. As we know, they are being phased out—but they will be replaced in 2019, pursuant to the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA), by the Merit-Based Incentive Payment System which will potentially introduce even more measures.
One expert who does not believe that MACRA will introduce a better way of linking measurement of physician performance to the amount of Medicare payments—because the concept of measurement as the best route to improvement is flawed—is Robert Berenson, MD, former chair of the Medicare Payment Advisory Commission (MedPAC) and former acting CMS administrator:
[Dr. Berenson] argues that the Medicare Access and CHIP Reauthorization Act (MACRA), which will steadily increase the amount of Medicare payments to physicians that are based on measures of value, will likely turn out to be “a doomed attempt to measure value.” “Practical challenges aside, pay for performance for health professionals may simply be a bad idea. Behavioral economists find that tangible rewards can undermine motivation for tasks that are intrinsically interesting or rewarding. Furthermore, such rewards have their strongest negative impact when they are perceived as being large, controlling, contingent on very specific task performance, or associated with surveillance, deadlines, or threats …”
Many of our readers would surely agree that pay for performance, the impetus for the explosion of quality measurement systems, “may simply be a bad idea.” Yul Ejnes, MD, a past chair of the American College of Physicians, wrote for the KevinMD blog (Let’s Fix Performance Measurement for Physicians, March 2, 2016):
It was supposed to be that if we provided high-quality care to our patients, the measurements would reflect that. Instead, the mantra is that if we score well on our measures, then that means that we provided high-quality care. In other words, the cart has become the horse. It’s time to fix that.
That is a concise and profound statement of the problem, and it is indeed “time to fix that.”
Recent media coverage of surgeons operating in two concurrent cases raises three issues: (1) patient safety, (2) compliance with the Medicare teaching physician billing rules and (3) transparency vis-à-vis patients.
The Safety Controversy
The question whether it is right or safe for surgeons to run two operations at once erupted publicly last year when the Boston Globe published a detailed report (Clash in the Name of Care) focusing on events that had occurred at Massachusetts General Hospital (MGH) in August 2012. A 41-year old patient had undergone complicated spinal surgery from which he emerged a quadriplegic, and it revealed itself that his surgeon had been in and out of the operating room, attending to a patient undergoing spinal fusion in another OR for seven of the eleven hours that the first case took to complete.
A controversy among MGH surgeons and anesthesiologists over concurrent surgeries had been years in the making. “A small but determined cohort of anesthesiologists and other Mass. General employees complained about at least 44 alleged problems involving concurrent surgeries,” the Globe article reported. Approximately three percent, or 1,000 cases annually, at MGH involved at least one patient with an open incision while a second case was underway. In the orthopedics department, however, 25 percent of cases overlapped. MGH denied all the allegations.
The senior hip and knee surgeon who had led the opposition to the practice—which he had been challenging for a decade—gave the Globe copies of internal hospital documents, with information that could identify patients removed, and he was quickly fired for being disruptive. After the dismissal, MGH conducted a review of 25 concurrent surgeries that had had complications and reported that none of the complications was due to the double-booking. The hospital also engaged a former federal prosecutor to investigate and he allegedly reported that there was nothing wrong with the practice of running cases concurrently. (Rappleye E. Concurrent surgeries cause conflict at MGH: 10 things to know. Beckers Hospital Review online, October 27, 2015).
The opposition leader alerted the Massachusetts Department of Health, which investigated and found nothing amiss at MGH, although several surgeons individually, including the one who operated on the paralyzed patient, remain under investigation.
In January of this year, the Massachusetts Board of Registration in Medicine approved a new regulation that would require surgeons to document each time they leave and enter the OR. It would also require that the primary surgeon identify the backup surgeon who would assume responsibility if the first surgeon left the room. Several state agencies must approve the regulations before they can go into effect at the end of March. (State acts on simultaneous surgeries. Boston Globe, January 7, 2016).
The US Attorney’s fraud unit, together with the Massachusetts Attorney General’s office, subpoenaed 10 years of internal records from MGH last November. During the summer, they interviewed several critics of double-booking, including the surgeon who was subsequently dismissed. (See below for a discussion of the potential fraud issues.)
The US Senate Finance Committee, which has jurisdiction over Medicare and is headed by Sen. Orrin Hatch (R-UT), is investigating the subject of concurrent surgical cases. Representatives of the American College of Surgeons (ACS) met with Committee staff on March 10, 2016. An ACS panel is in the final stages of drafting guidelines. One of the panel members told Globe reporters that “the new guidelines will allow for small overlaps, such as when an OR team is closing a surgical wound in one room and the attending surgeon is starting a second operation in another room, but not simultaneous surgeries.” Twenty hospitals, including MGH and the Cleveland Clinic, have received letters from the Committee requesting information on the frequency and safety of their use of the practice, and especially on patients’ knowledge and consequently their ability to give informed consent. (Overlapping surgeries to face US Senate inquiry. Boston Globe, March 13.) No hearings have been scheduled yet.
The practice of concurrent surgeries is “common at some hospitals, restricted or banned at others, but seldom studied or discussed publicly,” according to a follow-up column in the Boston Globe (MGH records sought in double-booking review, November 14, 2015). Is it safe? One way to answer that question is to look at malpractice data. The Doctors Company reviewed 7,330 surgery malpractice cases in its database for the eight-year period 2007-2015 and found no mention of concurrent surgery as a factor. Robin Diamond, MSN, JD, RN, Senior Vice President, Patient Safety and Risk Management at The Doctors Company sees the potential for future litigation, however, and recommends that hospitals have policies that:
Limit the surgeons permitted to perform concurrent surgeries to experienced physicians who have been deemed competent and have been privileged to do overlapping cases (Peter Dunbar, MD, of the Department of Anesthesiology at the University of Washington told us in a personal communication that the privilege must be carefully managed to deal with “over-confident surgeons who are inclined to do as many cases as possible and will very likely push the envelope”);
Limit the extent to which procedures can overlap;
Require a reason why concurrent surgeries are necessary. “Busy OR schedules can be justification enough, Diamond says, but there should be some reason beyond the surgeon simply wanting to double up and get out of the hospital sooner;”
Require full disclosure to the patient as part of the informed consent process;
Document the surgeon’s exit and return times in the OR record;
Define the requirement (if any) that a supervising or attending surgeon be “immediately available” to respond if the primary surgeon is out of the room, and
Ensure good patient handoff procedures.
Karen S. Sibert, MD, who recently returned to an academic setting from private anesthesiology practice in Los Angeles, gave her perspective in her blog post Running Two ORs: Is it always wrong? on November 7, 2015. Dr. Sibert answers her own question with an emphatic “no.” She has never “seen a patient come to harm because the surgeon scheduled concurrent cases.” It is not efficient to have a surgeon present while the anesthesiologist and the OR team are preparing the patient or the resident or fellow is closing the wound and the team is finishing the case:
Everything goes more smoothly when the surgeon is happily occupied in the case next door. … Often, the team is more efficient and at ease when the surgeon is occupied elsewhere while the patient wakes up and everything is done to move the patient safely out of the operating room. Then the operating room must be thoroughly scrubbed down before set-up can begin for the next case.
Dr. Sibert is unequivocal regarding the safety and efficiency of having the surgeon performing the critical portions of the first case while the second patient is being prepared—the scenario where “Once the critical work of the first case is complete, the surgeon can leave safely to begin work on the second one." Moreover, it would be difficult to train new surgeons without giving them the opportunity to perform cases themselves, under appropriate supervision. But Dr. Sibert is less convinced that long spine cases such as the ones that gave rise to so much attention at MGH, which typically require the surgeon to move back and forth between two ORs to attend to key portions of both, should be scheduled concurrently:
It would depend on the specific situation. In surgical groups where partners have comparable skill and experience, it often doesn’t matter much which surgeon is listed as the primary surgeon and which one is listed as the assistant. They may work together consistently, and when they run two rooms, the quality of care is no different.
Sometimes, however, it does matter whether the surgeon is busy with critical portions of one case when he or she is needed in the other OR—the overlap is not good for the patient or the team. The dissidents at MGH cited “cases where surgeons didn’t show up to operations, leaving the work to a resident or fellow; cases of patients lying under anesthesia for prolonged periods waiting for a doctor to arrive or return; cases where operating room staff were confused about who would do the operation.”
Most of the teaching hospitals in Boston allow minor overlap of cases, but only a few permit doctors to run two surgical cases simultaneously over an extended period. Boston Medical Center only allows certain types of procedures to run concurrently, not including complex spinal surgery. The Brigham and Women’s Hospital says it does not permit cases to run simultaneously for more than an hour, except in emergencies. Such restrictions are in line with Medicare payment policy for teaching cases.
Compliance with Medicare Rules
Teaching anesthesiologists are familiar with the provision in the Medicare Claims Processing Manual (Chap. 12 Sec. 100.1.2.A.4) that covers the conditions for payment in concurrent resident cases:
To qualify for payment, the teaching anesthesiologist, or different anesthesiologists in the same anesthesia group, must be present during all critical or key portions of the anesthesia service or procedure involved. The teaching anesthesiologist (or another anesthesiologist with whom the teaching physician has entered into an arrangement) must be immediately available to furnish anesthesia services during the entire procedure. The documentation in the patient’s medical records must indicate the teaching physician’s presence during all critical or key portions of the anesthesia procedure and the immediate availability of another teaching anesthesiologist as necessary.
The corresponding provision for teaching surgeons is Section 100.1.2.A.2., which is more restrictive and does not allow surgeons to substitute in for each other:
In order to bill Medicare for two overlapping surgeries, the teaching surgeon must be present during the critical or key portions of both operations. Therefore, the critical or key portions may not take place at the same time. When all of the key portions of the initial procedure have been completed, the teaching surgeon may begin to become involved in a second procedure. The teaching surgeon must personally document in the medical record that he/she was physically present during the critical or key portion(s) of both procedures. When a teaching physician is not present during non-critical or non-key portions of the procedure and is participating in another surgical procedure, he/she must arrange for another qualified surgeon to immediately assist the resident in the other case should the need arise.
It is in light of this well-established Medicare payment rule that the U.S. Attorney will consider whether MGH can be charged with fraud. Much will depend, of course, on which portions of each procedure were “critical” or “key” and required the physical presence of the primary attending. Still, by stating that “When all of the key portions of the initial procedure have been completed, the teaching surgeon may begin to become involved in a second procedure,” Medicare makes it difficult to argue that the surgeon can go back and forth between concurrent cases as he or she judges appropriate. The key portions of the first case must be completed before the surgeon becomes involved in another procedure.
Disclosure to Patients and Informed Consent
As noted above, a major focus of the Senate Finance Committee’s investigation is disclosure to the patient and informed consent. Patients who know that their surgeon is going to be involved in other cases concurrently with their own might withhold their consent to the procedure, and therefore the potential concurrency is a material fact. The letter to the 20 hospitals asks specifically whether they tell their patients that their operations will be performed concurrently. Sen. Hatch wrote: “We are concerned about reports of patients not being informed that they may be sharing their surgeon with another patient, and we are especially concerned by reports that, in some cases, steps have been taken to actively conceal this practice from patients.’’
The new regulation approved by the Massachusetts Board of Registration in Medicine would require surgeons to document each time they leave and enter the OR. This would certainly make it easier for patients with adverse outcomes to prove that their primary surgeon was not in attendance at critical moments. A documentation requirement might by its nature discourage the practice of running concurrent cases—with good or ill consequences; see Dr. Sibert’s blog entry, which states that “of course” patients should “be told that surgeons have scheduled two operating rooms.”
In this era of transparency and of sensitivity to the patient experience, the benefits to be garnered by fully informing patients of who will be in the OR taking care of them throughout their procedures outweigh any possible advantages of non-disclosure.
The saga is not yet over—although MGH has put in place a new policy on concurrent surgeries; the orthopedic surgeon who has been sued by his quadriplegic patient who moved to Stanford last November, and the surgeon who brought the information to the Globe is now retired. Anesthesiologists in some institutions will likely exercise heightened care to delay inducing anesthesia until they know when the surgeon will have completed all critical portions of his or her preceding case. The public and professional attention that the issue has received ensure that discussions will continue as new policies take shape.
The anesthesia record, like medical records in general, should be complete and accurate at the time when the physician signs it—ideally. In practice, it occasionally requires amendment. Given the huge role that accurate documentation plays in our medical payment system, compliance with the rules and regulations governing medical record amendments is important. Altered medical records have great potential for fraud, especially if the added information helps to raise the level of a billable service, and no one should be surprised if auditors look at any changes closely.
One basic principle was added to the first paragraph of the provision that regulates amendments in Chapter 3 of the Medicare Program Integrity Manual, Section 3.3.2.5, when that provision was updated effective October 2, 2015. The intent of the new paragraph is to make it clear that amendment should be the exception.
All services provided to beneficiaries are expected to be documented in the medical record at the time they are rendered. Occasionally, certain entries related to services provided are not properly documented. In this event, the documentation will need to be amended, corrected, or entered after rendering the service.
Section 3.3.2.5 further sets forth three “Recordkeeping Principles” that practices must follow in submitting amended documents to their Medicare carriers or auditors, and these apply to both paper and electronic health records (EHRs). Documents containing amendments must:
Clearly and permanently identify any amendment, correction or delayed entry as such, and
Clearly indicate the date and author of any amendment, correction or delayed entry, and
Clearly identify all original content, without deletion.
The Program Integrity Manual provision elaborates on paper vs. EHRs:
Paper Medical Records: When correcting a paper medical record, these principles are generally accomplished by:
Using a single line strike through so the original content is still readable, and
The author of the alteration must sign and date the revision.
Amendments or delayed entries to paper records must be clearly signed and dated upon entry into the record. Amendments or delayed entries to paper records may be initialed and dated if the medical record contains evidence associating the provider’s initials with their name.
Electronic Health Records (EHR): Medical record keeping within an EHR deserves special considerations; however, the principles specified above remain fundamental and necessary for document submission to MACs, CERT, Recovery Auditors, and ZPICs. Records sourced from electronic systems containing amendments, corrections or delayed entries must:
Distinctly identify any amendment, correction or delayed entry, and
Provide a reliable means to clearly identify the original content, the modified content, and the date and authorship of each modification of the record.
There are three legitimate types of amendment to a medical record: late entries, addenda and corrections. As explained on the website of Noridian Healthcare Solutions, the Medicare Administrative Contractor (MAC) for a number of Western states, the purposes and some particulars of the three types are:
Late Entry: A late entry supplies additional information that was omitted from the original entry. The late entry bears the current date, is added as soon as possible, is written only if the person documenting has total recall of the omitted information and signs the late entry.
Example: A late entry following treatment of multiple trauma might add: "The left foot was noted to be abraded laterally. John Doe MD 06/15/09"
Addendum: An addendum is used to provide information that was not available at the time of the original entry. The addendum should also be timely and bear the current date and reason for the addition or clarification of information being added to the medical record and be signed by the person making the addendum.
Example: An addendum could note: "The chest x-ray report was reviewed and showed an enlarged cardiac silhouette. John Doe MD 06/15/09"
Correction: When making a correction to the medical record, never write over, or otherwise obliterate the passage when an entry to a medical record is made in error. Draw a single line through the erroneous information, keeping the original entry legible. Sign or initial and date the deletion, stating the reason for correction above or in the margin. Document the correct information on the next line or space with the current date and time, making reference back to the original entry.
Correction of electronic records should follow the same principles of tracking both the original entry and the correction with the current date, time, reason for the change and initials of person making the correction. When a hard copy is generated from an electronic record, both records must show the correction. Any corrected record submitted must make clear the specific change made, the date of the change, and the identity of the person making that entry. (Emphasis in original.)
The following, on the other hand, are examples of amendments that may be considered deliberate falsification of medical records, a felony offense:
Creation of new records when records are requested
Back-dating entries
Post-dating entries
Pre-dating entries
Writing over, or
Adding to existing documentation (except as described in late entries, addendums and corrections)
A question that arises frequently concerns the timeliness of amendments to medical records. The Program Integrity Manual is oddly silent on the issue. Accordingly, physicians and their staff should complete any amendments in a reasonable time frame.
In brief, addenda, delayed entries or corrections to the medical or anesthesia record on which a Medicare claim is based must make it clear that they are created after the record is completed—that they are amendments. The must also clearly indicate their date and their author, and they "must clearly identify all original content, without deletion.” They should not be made routinely and generally they should be made only within a reasonable period after the date of service.
Hospitals and health systems may have their own policies and requirements, which physicians on the medical staff should also respect. We are not aware of any published private payer policies on medical record amendments but it is hard to imagine that they would be more rigorous than Medicare’s. In the interest of as much simplicity as possible, it might be best to follow Section 3.2.2.5 of the Program Integrity Manual for all payers.
One important voice sounding a warning or at least a heads-up about what is coming is that of Mark Weiss, Esq. The title of Mr. Weiss’s article— Impending Death of Hospitals: Will Your Anesthesia Practice Survive?—which is also the title of his forthcoming book—is intentionally provocative. He lays out several of the major threats confronting hospitals, starting with health system growth, through mergers and acquisitions, acquisition of physician practices and investments in integrated delivery networks. Others have predicted that the Federal Trade Commission will place a damper on hospital merger activity in 2016, but the quest for greater scale and scope is going to continue. Anesthesiologists may want to consider the wisdom of relying on the ongoing health of just one or two hospitals. This is especially true in light of the ability of physician-owned facilities, notably ambulatory surgery centers, and new technologies (think telemedicine) to disrupt hospitals’ traditional business. Mr. Weiss concludes in no uncertain terms that anesthesiologists who are not yet deeply engaged with freestanding facility care should turn in that direction.
Of course, with more than 5,600 licensed hospitals in the U.S., the need and opportunity for anesthesiologists in hospitals is not going to dissipate completely in the near future. In the Fall 2015 issue of The Communiqué, Rick Bushnell, MD, MBA explained why forming a perioperative surgical home (PSH) with the active support of the hospital was right for his group. He brings us up-to-date on the process of agreeing upon goals, priorities and resources that has led to the formation of a true partnership in his new article The Perioperative Surgical Home: Our Partnership with the C-Suite.
Jerry Ippolito, MBA, MHSA reminds us all of the continuous need to attend to the well-being of one’s hospital and surgeons in The Hospital is Your Practice’s Client—Understand Client Satisfaction to Retain Your Contract. As Mr. Ippolito states, “Every business, regardless of its service offering or discipline, must continue to reinvent itself, to remain marketable, in changing times. Anesthesia is no exception.”
The arrival of a new year always brings us coding changes. Kelly Dennis, MBA, who is a certified expert coder with 32 years of experience in anesthesia, reviews the changes to the CPT® system and also to the increasingly frustrating Physician Quality Reporting System (PQRS) in 2016 Coding Updates for Anesthesia. PQRS is now in its penultimate year of existence, and we would like to think that the Merit- Based Incentive Payment System that, in 2019, will replace the various Medicare quality reporting programs bedeviling us today will be an improvement. We shall see.
Confidentiality is a topic that perennially looms large in healthcare. Improving or even maintaining health does not take place in a void; information is and must be shared in order to achieve our health-related goals both as individuals and as participants in healthcare systems. One area that engenders confusion is the extent to which personal information gathered and shared in the context of peer review may be protected from disclosure or “discovery” in legal proceedings. Every state has a statute governing the discoverability of records, reports and conclusions. In Confidentiality in the Peer Review Process: What Does it Mean and What is Covered? Part I, Neda Ryan, Esq. reminds readers of the basic principles and considerations and also provides a summary of the statutes for Alabama through Iowa. Part II will appear in the Spring issue of The Communiqué and will contain summaries for the remaining states.
Just as important a legal matter, although one that comes up somewhat less frequently than confidentiality, is covered by Kathryn Hickner, Esq. in “I’m Out Of Here!” Now What? Physicians leaving a practice are often covered by an employment contract with Image may be NSFW. Clik here to view.the group they are leaving and also by federal and state laws regarding employer benefit
Many pain medicine procedures, and, increasingly, perioperative and critical care procedures such as central venous access are performed using ultrasound guidance (U/S). Indeed, U/S is an integral part of many CPT® codes, e.g., 20604 [Arthrocentesis, aspiration and/or injection, small joint or bursa, (e.g., fingers, toes), with ultrasound guidance, with permanent recording and reporting]. When and where, and by whom, must those permanent images be stored? What if another entity, such as a hospital, is responsible for storing them? According to Sonosite,
All diagnostic ultrasound examinations, including those when ultrasound is used to guide a procedure, require that permanently recorded images be maintained in the patient record. The images can be kept in the patient record or some other archive--they do not need to be submitted with the claim. Images can be stored as printed images, on a tape or electronic medium. Documentation of the study must be available to the insurer upon request. A written report of all ultrasound studies should be maintained in the patient's record. In the case of ultrasound guidance, the written report may be filed as a separate item in the patient’s record or it may be included within the report of the procedure for which the guidance is utilized.
Adequate documentation is essential for high-quality patient care, should be performed in accordance with the AIUM Practice Parameter for Documentation of an Ultrasound Examination, and should be permanently documented in the patient’s medical record. Retention of the ultrasound examination should be consistent both with clinical needs and with relevant legal and local health care facility requirements. The procedure documentation should include the following:
[1.-11. Omitted] 12. Preprocedure, intraprocedure, and postprocedure still image(s) or videos:
a. Images should be labeled with the patient identification, facility identification, procedure date, and side (right or left) of the procedure site. b. Inclusion of at least one image demonstrating the needle or device placed into the target region is required unless the indirect technique is used (see section VI. Specifications for Ultrasound-Guided Joint Aspirations and Injections). c. All images should be permanently archived and easily retrievable. d. Variations from normal size or morphology should be recorded and accompanied by measurements.
Hospitals that participate in the Medicare program are required by regulations to retain imaging report copies and printouts, films, scans and other radiologic services image records for five years. (42 CFR 482.26(d)). Some states follow federal regulations, but many require that providers store images for several years longer, or have stricter standards for minors.
Most state statutes address hospitals and other facilities but a few, for example Indiana and Maryland, place the responsibility directly on physicians. A five-year minimum retention period is the most common, but there is variation. New Hampshire, for example, provides that “Both hospitals and health facilities must retain medical records of adults for a period of seven years from discharge. Children’s records must be retained to the age of majority plus seven years, and X-ray film must be stored at least seven years. The rules for each state are summarized in a table prepared by the American Healthcare Information Management Association.
Thus most states do not require physicians to retain medical records for a specific period of time. Nor does the HIPAA Privacy Rule, although it does mandate “that covered entities apply appropriate administrative, technical, and physical safeguards to protect the privacy of medical records and other protected health information (PHI) for whatever period such information is maintained by a covered entity, including through disposal.” (See 45 CFR 164.530(c)). The statutes of limitations under federal and state fraud statutes can be considered as setting a minimum time period for retention of medical records that might be relevant in a Medicare or Medicaid fraud investigation. For Medicaid and Medicare fraud, federal law establishes (1) a civil statute of limitations of six years (42 U.S.C. § 1320a-7a(c)(1)) and (2) a criminal statute of limitations of five years (18 U.S.C. § 3282).
Physicians have an obligation to retain patient records which may reasonably be of value to a patient. The following guidelines are offered to assist physicians in meeting their ethical and legal obligations:
(1) Medical considerations are the primary basis for deciding how long to retain medical records. For example, operative notes and chemotherapy records should always be part of the patient’s chart. In deciding whether to keep certain parts of the record, an appropriate criterion is whether a physician would want the information if he or she were seeing the patient for the first time. (2) If a particular record no longer needs to be kept for medical reasons, the physician should check state laws to see if there is a requirement that records be kept for a minimum length of time. Most states will not have such a provision. If they do, it will be part of the statutory code or state licensing board. (3) In all cases, medical records should be kept for at least as long as the length of time of the statute of limitations for medical malpractice claims. The statute of limitations may be three or more years, depending on the state law. State medical associations and insurance carriers are the best resources for this information. (4) Whatever the statute of limitations, a physician should measure time from the last professional contact with the patient. (5) If a patient is a minor, the statute of limitations for medical malpractice claims may not apply until the patient reaches the age of majority. (6) Immunization records always must be kept. (7) The records of any patient covered by Medicare or Medicaid must be kept at least five years.
Thus we have seen that the permanent image is a part of the medical record and that the physician (as well as the hospital) should retain the medical record for a certain period of time, generally no shorter than the applicable malpractice or fraud statute of limitations. What if the physician or patient needs access to a part of the medical record that is in the exclusive possession of the hospital—for example, an U/S image?
There should be no problem if the request for the image is made within the statutory period during which the hospital or other facility must retain the medical record. The Medicare Conditions of Participation provide in this regard (42 CFR 482.24):
The hospital must have a medical record service that has administrative responsibility for medical records. A medical record must be maintained for every individual evaluated or treated in the hospital.
(a) Standard: Organization and staffing. The organization of the medical record service must be appropriate to the scope and complexity of the services performed. The hospital must employ adequate personnel to ensure prompt completion, filing, and retrieval of records.
Sometimes hospitals fall short of this standard. About 600 million imaging procedures are performed each year by health-care providers in the U.S., including CT scans, X-rays, ultrasounds and MRIs. (Landro L. Where Do You Keep All Those Images? Wall Street Journal, April 8, 2013). It is inevitable that some records will get lost and that a hospital will not be able to produce them for the physician who is facing an audit or a malpractice lawsuit. The patient and/or the physician may have grounds for a lawsuit against the hospital, depending on the state in which they are located—and depending on whether the hospital’s obligation to keep and produce records is stipulated in a contract.
Consider including provisions in your hospital service contracts that require the facility to retain all radiological images for x number of years from the time the images are created, x being at least as long as the applicable statute of limitations. State that the hospital must give you the images within, e.g., 24, 48 or 72 hours from the time you request them. (The request will have to be sufficiently specific for the hospital to be able to identify the records). Include in the contract your right to indemnification if the hospital fails to deliver the documentation (the images) on time and your group is harmed by the breach. Such protection can be drafted in various ways. We have seen enough instances in which anesthesiology groups were unable to recover part of the patient record from the hospital to know that the protection may be important.
Merely including the hospital’s duty in the contract does not guarantee protection. The best strategy, from the anesthesiologists’ point of view, is to make the hospital aware from the outset that safeguarding the entire medical record is critically important—not just to comply with Medicare’s and The Joint Commission’s accreditation standards, but to immunize the hospital against the financial and legal consequences of losing the records. The group must be vigilant in making sure that the hospital is meeting its obligation. If the group knows that it is about to be audited or be the target of a malpractice action, then it should notify the hospital that the records at issue must be retained and not purged or destroyed.
Fortunately, storage space or the lack thereof is no longer an excuse. The U/S images, like so much else, can be stored conveniently in the cloud.
How would you like to know exactly what’s going to happen in the future so that you can prepare for and profit from it?
I have a crystal ball. Here, let me share it with you.
We’re going to review some of the trends currently impacting, and soon to impact, hospitals that will, I predict, lead to their destruction, at least as we know them.
There is absolutely no question that these trends are going to have an impact on your anesthesia practice. Start preparing now.
Trend 1: Hospitals Are Getting Bigger and That is a Weakness
Government induces physician labor
Image may be NSFW. Clik here to view.Obamacare favors the growth of hospitals with its incentives for aligning physicians. Think Accountable Care Organizations (ACOs) and other incentives to coordinate care, meaning coordination via hospitals.
Although reports lag by several years, at least 20 percent to 30 percent of all practicing physicians are currently employed by hospitals. There was a 34 percent increase in hospital employment of physicians between 2000 and 2010.
In addition, an uncertain number of physicians, very likely a significant number of them, are controlled by hospitals through alignment relationships such as ACOs and foundation model medical groups.
Hospital merger mania
As hospitals gobbled up physician practices, hospitals began gobbling each other up as well.
In 2013 there were 105 hospital mergers. In 2014 there were fewer, approximately 100. Overall, since 2010, there has been a 44 percent increase in the pace of hospital mergers.
Hospitals merge because they think that there’s strength in a larger entity. In other words, they believe that it brings so-called economies of scale. If that means that two hospitals merge and become one, and then one facility closes down, perhaps that’s the case. But that’s not the general trend. Instead, mergers are often used to build bigger hospital systems in which there are little to no economies of scale. It’s often the case that when large entities merge, administrative costs go up.
In the 1990s, there was a similar wave of hospital mergers. Most merged hospitals failed. The same argument about economies of scale was made then: that merging would cut costs. But it didn’t turn out to be true.
Hospitals are losing the economic bet on employed physicians
Image may be NSFW. Clik here to view.A 2014 study by the Kentucky hospital industry revealed that the cost to hospitals of employing physicians is increasing.
A majority of hospitals reported increasing losses per physician; on average more than $100,000 per employee and, for some specialists, more than $200,000 per employee.
The larger the hospital and the larger the hospital system, the larger the losses.
Hospitals are losing the bet on integrated delivery networks
And, as to quality, a large study by the National Academy of Social Insurance “found little evidence that integrated delivery networks have reduced costs or improved the quality of care.”
Fragility will lead to cascading failure
In the 1990s, if a hospital failed, chances were it failed alone. In other words, the physician practices associated with that facility were independent. Certainly, office-based physicians found privileges at another facility. Hospital-based physicians were impacted disproportionately in comparison to their office-based colleagues, but at least there were other hospitals to which to expand their services.
But now, if a hospital or a merger-bloated hospital system with its employed or otherwise tightly affiliated physicians fails, all of those physicians are out of a job.
So we have merger for the cure of high costs. And we have a history from the 1990s of a similar trend that resulted in the failure to cut costs resulting in hospital failures. But as opposed to what happened in the 1990s, today many of these merged hospitals not only have traditional hospital-side expenses, they have taken on the huge expenses of employing physicians. Note that’s not just physician labor expense, but the complete expense of operating the practices, from space to equipment to supplies to billing to staff and so on.
Trend 2: Physician-Owned Facilities
The growth of physician-owned facilities is a key disruptor of the traditional hospital business, shifting cases out of hospitals.
Ambulatory Surgery Centers
Image may be NSFW. Clik here to view.Ambulatory surgery centers (ASCs) pull cases—generally the better reimbursed cases—out of the hospital O.R. They offer a significantly cheaper alternative to Medicare, private payors and patients. They also make money for their physician owners.
Currently, there are nearly 6,000 ASCs in the United States. There has been a slowdown in the net addition of ASCs during the last two years. In large part this is due to the fact that hospitals are attempting to remove the competition by purchasing ASCs in the local market, closing some and converting others to hospital outpatient departments (HOPD).
Notwithstanding that buying spree, it’s unlikely that hospitals will be able to stop the shift of cases to the ASC setting.
Procedures that only a few years ago were inpatient are now being performed on an outpatient basis. And, in some specialties, new surgical codes enable cases to be brought to ASCs, thus opening the specialty to fostering ASC development.
HOPD payment differential will backfire
Although recent federal budget legislation has reduced some of the benefit of operating an outpatient facility as a HOPD sooner or later the payment differential will play itself out to disrupt hospitals’ futures. There’s little justification for paying more to hospitals for the same procedure that can be performed in a hospital-free, that is, ASC, setting.
But even if the differential continues to be paid, physicians will continue to invest in and take cases to ASCs and payors will continue to want access to their more cost efficient services.
It’s unlikely that hospitals will be able to garner the political support to put the same roadblocks on ASCs that they’ve managed to place on physician-owned hospitals.
Physician-owned hospitals
In order to protect their near monopoly, the investor-owned and non-taxpaying hospitals (many of which are busy employing and otherwise aligning physicians) have claimed that if physicians own hospitals in order to create teamwork and provide coordinated care, that is bad. But if hospitals own physicians in order to create teamwork and provide coordinated care, that is good.
This nonsensical argument will eventually lose traction.
Even if physicians are prevented from owning hospitals that qualify to treat federal healthcare program cases, they will continue to invest in smaller facilities focused on private payor cases. They will be able to avoid the low reimbursement that comes from governmental programs and the “no reimbursement” that comes from complete charity care.
Trend 3: New Classes of Competitors
New business models are disrupting the flow of patients, patients who were formerly destined to be referred into a hospital’s “world.”
Walk right in
These models include walk-in clinics of the type opening at retail stores such as Walgreen’s, Rite Aid and CVS. In fact, CVS, until recently known as CVS Pharmacy, is now known as CVS Healthcare, which is a clear indication of where they believe healthcare is going.
Other examples are the plethora of walk-in and urgent care facilities built in strip centers and other ease-of-access locations. In fact, in Colorado, Texas and a number of other states, free-standing emergency rooms—often located near or at intersections close to acute care hospitals—syphon off patients headed to the hospital’s OR based on their accessibility and their near zero wait times.
The point here is that these types of facilities signal a trend: non-traditional ventures are disrupting the flow of patients to physicians’ offices and to hospital emergency rooms. More importantly, because this trend has an exponential impact, patients don’t have the same emotional barriers to obtaining medical care outside of the physician office or hospital setting that they had 20 years ago.
In other words, if care can be obtained in a less intense, less costly, more convenient setting, it’s not just insurance carriers who are going to push for it, it’s patients who are going to demand it.
Updated house calls
It’s 7:00 a.m. on a Wednesday morning and you feel like death warmed over. When you call your doctor’s office (not open until 8:30) you know that you’ll be told that they might be able to fit you in on Friday. You’re lucky, because the average waiting time in the U.S. works out to more than 18 days.
But why bother, especially when a growing number of services will send a physician or nurse practitioner to see you now, at a cost that’s probably one-third to one-half less than what your own physician would charge for an in-office appointment.
And, if you don’t have to see a physician, or even a nurse, in person, why see one? Why not stay at home and simply transmit the same information about your condition to a physician or another provider via telemedicine?
Image may be NSFW. Clik here to view.It’s not difficult to see that both house call services and telemedicine are disruptive to traditional medical practitioners. In fact, in some states, primary care physicians are exerting pressure on state regulators to make it more difficult for telemedicine and other telehealth companies to operate. Eventually those anticompetitive efforts will fail as patients demand those services. After all, pushing for regulation is the death gasp of any profession or industry; if they can’t compete on their own, they turn to the government, and especially to bureaucrats, to protect them.
It requires only slightly more foresight to realize that, in the end, those and other new classes of competitors will not only disrupt traditional office practice, they’ll disrupt hospitals as well.
Patients will no longer be following the normal route of (1) go to a primary care doctor in an office building on or near a hospital campus, (2) be referred by that physician to a specialist on staff at the same hospital for more detailed diagnosis and care and (3) receive diagnostic services and treatment at the hospital.
Trend 4: The Role of Technology
We’re at a technological tipping point and tech is the fuel for the fire of the demise of hospitals as we know them. For decades, the cost of technology in almost every industry other than healthcare, resulted in lower costs to the consumer. But in healthcare, all technology did was increase costs.
This history of technology also fed the growth of hospitals. Who, but large facilities, could afford to buy the technology? Wasn’t it cheaper and more efficient to, in essence, spread the cost of that technology by locating it in a central location, the hospital, for access by those in the community, both physicians and other providers, as well as by patients?
Thus came the centralizing of technology (read that as medical equipment) from imaging to monitoring to operating rooms themselves.
But today, the cost of technology has shifted. Instead of being more expensive, it is less. In fact, in many cases it’s become so much less that it is, or soon will be, affordable at the consumer level, bypassing completely the ASC and physician level.
And, importantly, the size (sometimes there is, effectively, no size at all) of new equipment has shrunk.
Technology is quickly becoming the enabler for devices and for services that permit the disruption of the centuries-old doctor-patient relationship.
Star Trek in your home
Remember the “tricorder” from Star Trek, the handheld medical diagnostic device? Now, it’s time for the real one.
The Qualcomm Tricorder XPRIZE is a $10 million dollar prize for a tool capable of capturing key health metrics and diagnosing a set of 15 diseases. As of this writing, there are seven finalists.
Consider the OtoHOME device from Cellscope. It’s an iPhone device that allows parents to examine their child’s ears and record the result. It then connects them to a doctor for an immediate response. Dozens of other smartphone and wearable devices exist, each of which will reduce visits to traditional primary care doctors. Referrals to specialists (including all of those employed by hospitals) will be reduced, as will diagnostic procedures performed at hospitals.
Tech will also lead to less invasive surgery and to implantable devices that allay more surgery.
It’s also bound to lead to the fact that more procedures can be performed in either smaller, specialty hospitals or in outpatient settings. Hospitals will no longer need to provide everything to everyone. Procedures will move out of general hospitals into specialty ones and eventually will move out of hospitals altogether into ambulatory facilities.
The Bottom Line For Hospitals
Hospitals have expanded to become “full service” and have “bought” physicians to capture patients into the system. They claim that by closely aligning physicians they can deliver better care at a lower cost. But they are losing money on employed physicians and there’s no evidence that close alignment of physicians results in better care.
Image may be NSFW. Clik here to view.At the same time, patients are increasingly taking more control of their own diagnosis (and in some cases care) via technology.
Both technology and new classes of healthcare businesses (e.g., CVS Healthcare, Teladoc, etc.) are enabling patients to bypass traditional brick and mortar facilities (e.g., hospitals and physicians’ offices).
Patients don’t care as much as before whether they see a doctor, a nurse practitioner or some type of technician. And, for hospitals this is the big one, they don’t care as much if they obtain care from someone within the hospital’s patient acquisition funnel, or if they get surgery at an ASC or some other non-hospital site. As medicines improve (medicine as the future of surgery) and as miniaturization permits more procedures to be performed outside of the hospital, non-hospital facilities will syphon off a larger and larger percentage of hospital business.
Or perhaps patients won’t receive care at any facility—perhaps the facility will come to them: care in a “pod” inside or outside of your house?
Ultimate Hospital Bottom Line
Hospitals will shrink. They will be for the sickest people only. They might become monitoring stations for patients receiving care at home. Many will fail.
The Bottom Line For Anesthesiologists and CRNAs
If you think that hospital employment or close alignment is safe, think again.
Anesthesia groups can’t ever be dependent upon a single hospital relationship. In the past, the concern was that that facility might terminate your contract. In the near future, the concern will be that the hospital might not survive.
Certainly, some hospitals will survive but they will be only for the sickest patients and the most complicated procedures. There will continue to be some—reduced—need for anesthesia services at those facilities.
Ultimate Anesthesia Bottom Line
Freestanding facilities, even mobile ones, will be the future of the huge bulk of surgical care. If your practice isn’t already heavily focused on freestanding facility care, begin pivoting in that direction.
[Author’s Note: This article is an abridged adaptation of my upcoming book Impending Death of Hospitals: Why You Must Plan Your Medical Practice’s Survival, due to be released in early 2016.]
 vash, CHTSPW, of Koratek Perioperative Consulting, LLC takes a pragmatic look at anesthesia information management systems in her article Ensuring the Hospital’s AIMS Produces the Business Information Your Practice Needs. Whether your hospital is looking at a new AIMS implementation or already has an AIMS in place, there are steps you can take to make sure it turns the data captured by the system into the business information your practice needs.
vash, CHTSPW, of Koratek Perioperative Consulting, LLC takes a pragmatic look at anesthesia information management systems in her article Ensuring the Hospital’s AIMS Produces the Business Information Your Practice Needs. Whether your hospital is looking at a new AIMS implementation or already has an AIMS in place, there are steps you can take to make sure it turns the data captured by the system into the business information your practice needs.